
| JuHee Lee | 2 Articles |
Purpose
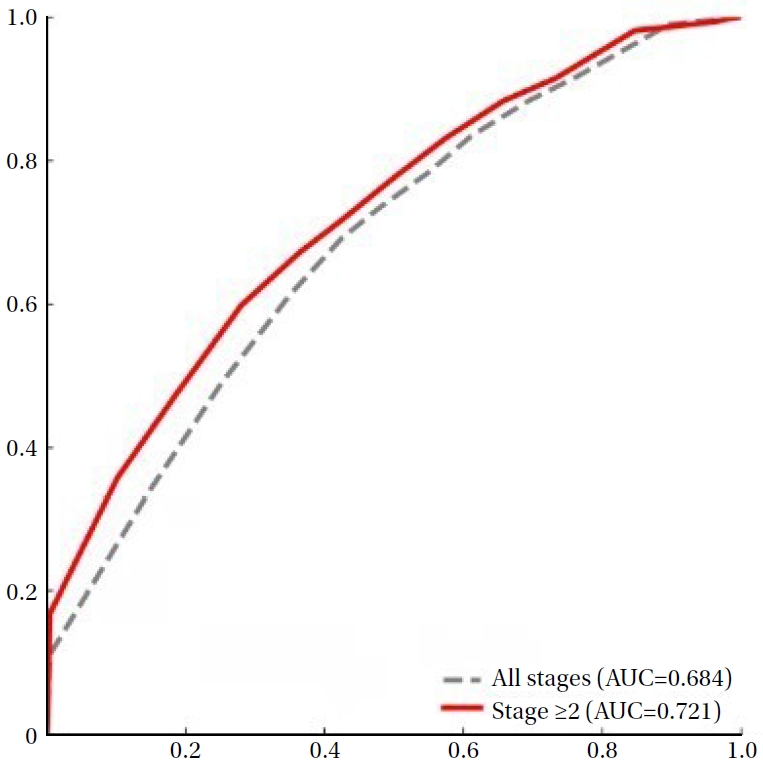
This study aimed to identify a clinically meaningful cut-off score on the Pressure Ulcer Scale for Healing tool for objectively determining healing in adult inpatients with pressure injury. Methods A retrospective analysis was conducted using electronic health records from adult inpatients at a tertiary hospital in South Korea. Pressure Ulcer Scale for Healing scores were calculated based on wound size, exudate amount, and tissue type. Receiver operating characteristic curve analyses were performed, and optimal cut-off scores were identified using the Youden Index. Stratified analyses by pressure injury stage were also conducted to evaluate predictive performance. Results A total of 20,476 pressure injuries were analyzed, of which 5,873 were classified as healed. Although all stages were initially included, stage 1 pressure injuries demonstrated limited discriminative ability (area under the curve=0.612) and were therefore excluded from cut-off derivation. For stage 2 or higher pressure injuries, the optimal cut-off score was 3.5, yielding an area under the curve of 0.721, with a sensitivity of 59.8% and a specificity of 72.0%. Conclusion The identified threshold for stage 2 or higher pressure injuries demonstrated meaningful discriminative ability for determining wound healing status. Application of this criterion may support more objective and consistent clinical decision-making when using the Pressure Ulcer Scale for Healing in nursing practice.
Purpose
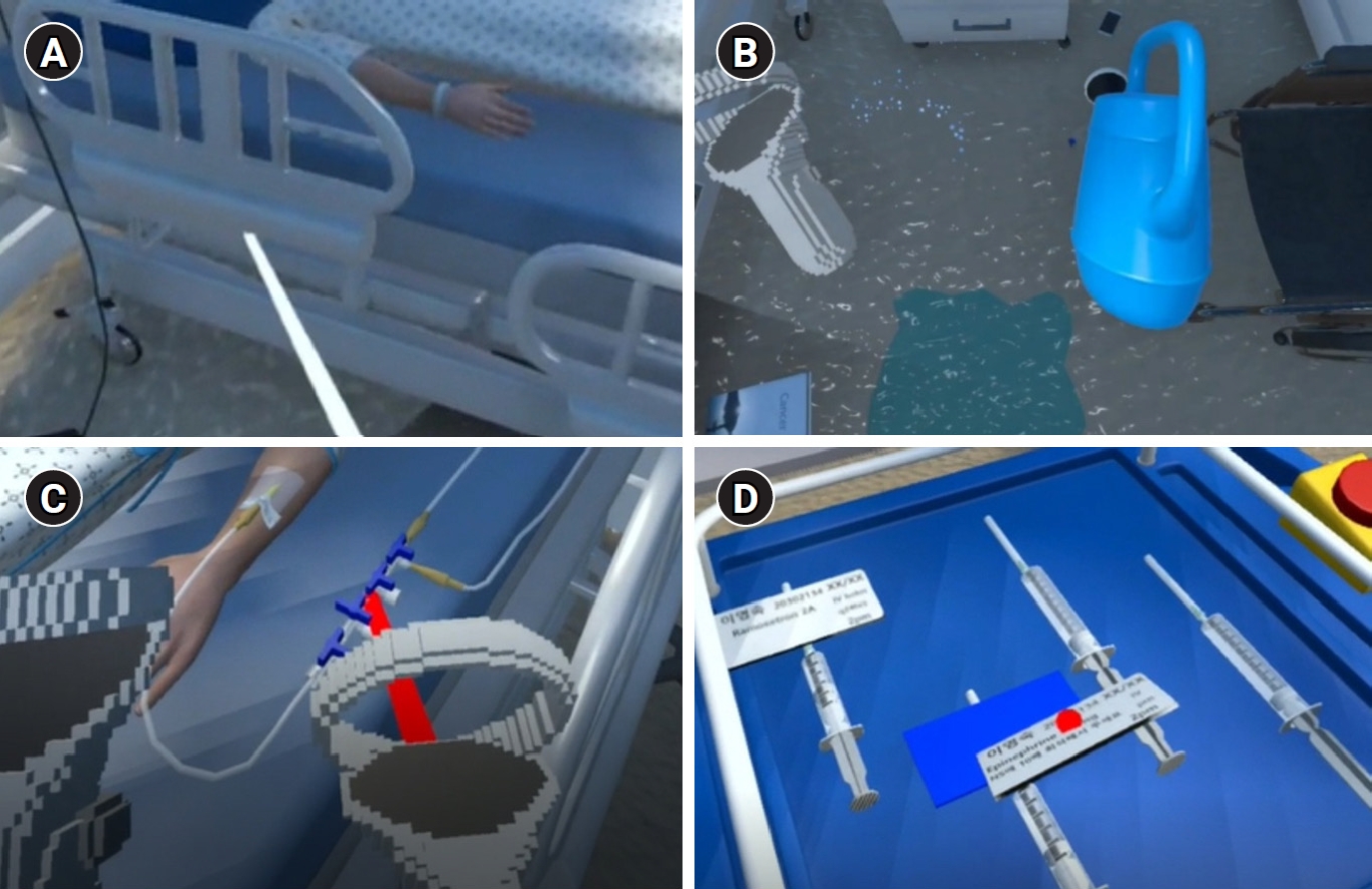
Falls and medication errors are the most common patient safety incidents globally. Kolb’s experiential learning theory supports the application of cognitive learning in clinical settings. This study examined the effectiveness of Experiential Learning–Based Fall and Medication Error Prevention Education (EFMPE), utilizing virtual reality and room of errors. Methods A randomized controlled trial was conducted with 28 fourth-year nursing students (15 experimental, 13 control). The experimental group participated in EFMPE from February 1 to 6, 2024, comprising six sessions of 2 hours each. The control group received traditional lectures. Safety control confidence and course interest were measured before and immediately after the intervention; safety control confidence was reassessed 6 weeks later. Results Both groups showed immediate improvement; however, only the experimental group sustained increased safety control confidence after 6 weeks (Wald χ²=13.21, p<.001). Course interest was significantly higher in the experimental group post-intervention (Wald χ²=10.64, p=.001). Conclusion These preliminary findings suggest that EFMPE potentially supports the prevention of falls and medication errors in clinical practice. Citations Citations to this article as recorded by
|
|
 E-SUBMISSION
E-SUBMISSION