Abstract
-
Purpose
This scoping review aimed to explore the characteristics and educational effects of game-based virtual reality (VR) programs used in nursing education, providing foundational insights for future instructional design and research.
-
Methods
Following the Joanna Briggs Institute guidelines and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews checklist, a comprehensive literature search was conducted across eight databases for studies published between April 2014 and March 2025. Studies were screened and selected using the population, concept, context framework. Twenty-four studies met the inclusion criteria and were analyzed.
-
Results
Most of the 24 included studies targeted nursing students, with some involving practicing nurses. Interventions primarily employed immersive VR head-mounted displays and incorporated diverse game elements such as mission-based scenarios, challenges, feedback loops, and virtual patient interactions. Educational effects were categorized into cognitive, affective, and psychomotor domains. Improvements in knowledge acquisition, self-efficacy, learning motivation, and skill performance were consistently reported. Additionally, most studies reported enhanced learner satisfaction, engagement, and emotional immersion. However, limited evidence was found regarding teamwork and communication skills.
-
Conclusion
Game-based VR programs show substantial potential as effective instructional strategies in nursing education. Their design features—including immediate feedback, repeatable immersive scenarios, and engaging game mechanics—support learner-centered and self-directed learning. Nevertheless, the current evidence base largely focuses on nursing students and short-term outcomes. Future studies should encompass diverse nursing populations and assess long-term effects and real-world applicability, particularly in team-based and clinical practice contexts.
-
Key Words: Education, nursing; Educational technology; Simulation training; Virtual reality
INTRODUCTION
With global changes in the healthcare environment, including population aging and the increasing prevalence of communicable and noncommunicable diseases, healthcare systems increasingly demand nursing personnel with advanced expertise [
1]. The World Health Organization [
2] identifies nurses as a central component in achieving universal health coverage, emphasizing the critical role of nursing education. In this context, nursing education is evolving beyond the simple transmission of knowledge to provide integrated learning experiences that foster the skills and critical thinking required in complex clinical environments [
3]. This underscores the need for instructional designs that strengthen learners’ confidence and clinical competence [
4], and highlights the importance of dynamic interactions among educators, learners, and institutional support systems in determining educational effectiveness [
5]. As the complexity and expectations of clinical practice continue to expand, innovative teaching and learning strategies are being actively pursued in nursing education. For instance, the widespread suspension of face-to-face classes and clinical practicums during the coronavirus disease 2019 (COVID-19) pandemic [
6] accelerated the exploration of alternative approaches that can maximize learning outcomes even in remote or hybrid settings.
In particular, virtual reality (VR) technology, by offering immersion, realism, and real-time interaction with the learning environment [
7], has gained recognition as a promising educational tool for enhancing the clinical competence of nursing students and practicing nurses [
8]. VR-based learning allows learners to safely experience diverse clinical scenarios that closely replicate real-world conditions [
9], and has been reported to positively affect knowledge, skill performance, critical thinking, self-efficacy, and learner satisfaction [
10,
11]. The opportunity to repeatedly practice complex and varied clinical situations helps reduce fear of failure and fosters learner confidence [
12].
Recently, game-based learning (GBL) and gamification—approaches that incorporate game design elements into instructional strategies—have received increasing attention as innovative methods to improve the effectiveness of nursing education. Gamification techniques that include elements such as points, leaderboards, and rewards [
13,
14] can stimulate engagement and sustain learner participation, ultimately maximizing educational outcomes. These approaches have demonstrated superiority over traditional teaching methods in enhancing knowledge retention, learning motivation, critical thinking, decision-making, academic achievement, and student engagement, while also promoting teamwork and social interaction among learners [
15]. Collectively, these findings indicate that gamification can serve as an effective instructional strategy in nursing education by encouraging active participation and supporting self-directed learning.
To date, a variety of game-based VR programs have been developed for nursing education across topics such as basic nursing skills [A2,A8,A12,A15,A23], infection control [A3,A7,A12], disaster nursing [A9,A10], and emotional empathy [A22,A24]. Researchers have also extensively investigated the educational effects of VR and GBL independently. For example, some studies have classified the purposes and implementation technologies of VR simulations in nursing education [
11], while others have conducted meta-analyses examining the effects of VR-based interventions on knowledge acquisition, skill proficiency, and learning satisfaction [
7,
16]. Similarly, systematic reviews have explored the influence of GBL on immersion and self-efficacy [
15,
17]. In Korea, several studies have assessed the outcomes of VR-based nursing education [
18] and the learning effects of gamification strategies [
19]. However, existing research has limitations in that it rarely integrates analyses of hybrid interventions combining VR and GBL. Most studies focus solely on nursing students and tend to emphasize outcome evaluations rather than the structural and design features of the interventions themselves.
Therefore, this study conducted a scoping review of intervention studies on game-based VR programs for nursing education published in domestic and international journals. The aim was to comprehensively analyze their characteristics, structural components, design features, and educational outcomes. Scoping reviews are particularly valuable for systematically identifying the range and trends of existing research on a specific topic and for proposing directions for future studies [
20]. Through this review, we sought to identify the educational topics and implementation methods of hybrid interventions that integrate VR and gamification, summarize their learning outcomes, and provide foundational evidence for the further development and application of game-based VR programs in nursing education.
METHODS
1. Study Design
A scoping review was conducted to identify the characteristics and educational effects of VR programs based on GBL for nursing students and nurses. The review followed the five-stage framework proposed by Arksey and O’Malley [
21]: (1) identifying the research question; (2) identifying relevant studies; (3) study selection; (4) charting the data; and (5) collating, summarizing, and reporting the results. The review process was guided by the methodology of the Joanna Briggs Institute (JBI) [
22], and reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [
23]. Both the JBI guidelines and PRISMA-ScR checklist were used throughout the review process. The protocol for this scoping review was registered on the Open Science Framework (OSF; DOI: 10.17605/OSF.IO/568BW).
To establish eligibility criteria for study selection, this scoping review applied the population, concept, and context framework recommended by the JBI [
22]. The population included nursing students and practicing nurses. Studies were eligible if participants directly engaged in interventions related to nursing education. The concept referred to the application of VR technology incorporating GBL elements as an educational intervention. Only studies integrating gamification or specific game elements within VR programs were included. The context comprised nursing education settings that employed game-based VR programs to improve learning outcomes, skill acquisition, or learning motivation. Studies were eligible if they addressed educational topics such as nursing theory, clinical skills, or clinical decision-making, provided that the educational objectives were explicitly stated. Based on these criteria, the primary research question guiding this study was: “What are the educational characteristics and learning outcomes of game-based VR programs applied to nursing students and nurses?”
The literature search for this scoping review was conducted in April 2025. With the release of the Oculus Rift in 2013, head-mounted display (HMD)-based VR entered full-scale commercialization, making its use feasible in educational contexts [
24,
25]. Around 2014, research in healthcare education began to expand rapidly [
26,
27]. Therefore, to capture recent trends, this review searched for studies published in domestic and international journals between April 2014 and March 2025. The international databases searched were PubMed, the Cumulative Index to Nursing and Allied Health Literature (CINAHL), the Cochrane Central Register of Controlled Trials (CENTRAL), and Excerpta Medica (EMBASE).
Search terms for international databases combined the following: (1) “Students,” “Nursing,” “undergraduate nursing student,” “Nurs*,” “Nursing student*,” “School Nursing,” or “Nurse”; (2) “Education” or “Learning”; (3) “Game,” “Game-based,” or “Gamification”; and (4) “Virtual Reality” or “VR.”
For Korean literature, the databases RISS, KISS, DBpia, and KMbase were searched. The search terms used internationally were adapted to suit the search functions of these databases. Korean search combinations included: (1) “nursing student,” “undergraduate nursing student,” or “nurse”; (2) “nursing,” “nursing education,” “education,” or “learning”; (3) “gamification,” “game-based,” or “game”; and (4) “virtual reality” (
Supplementary Table 1).
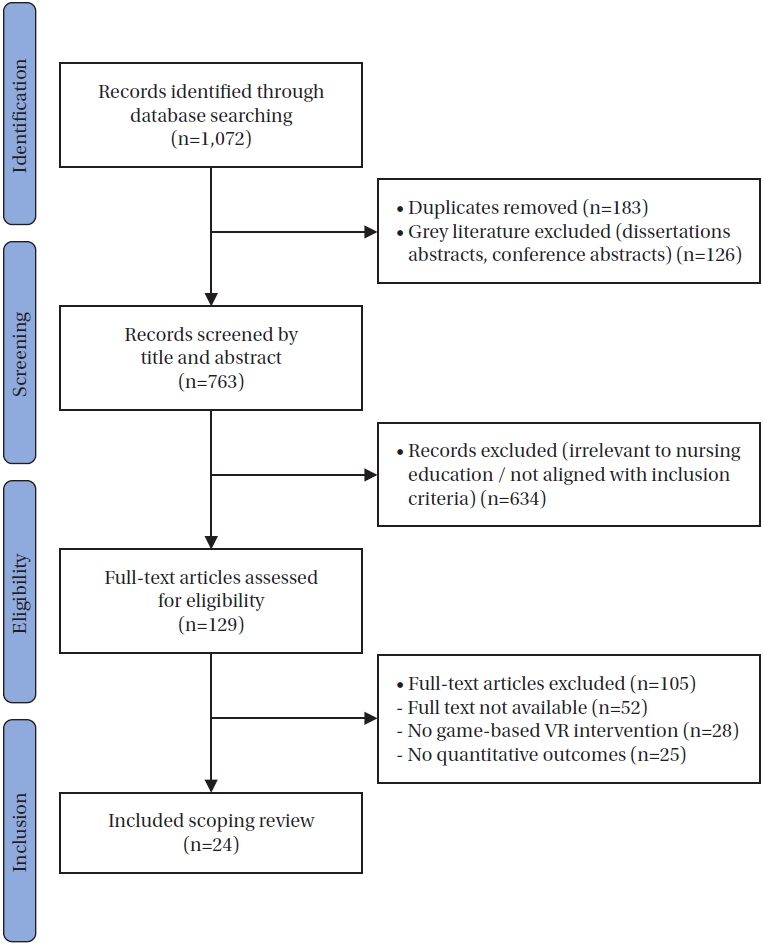
This scoping review included studies that investigated the characteristics and educational effects of game-based VR programs in nursing education for both nursing students and practicing nurses. Eligible studies implemented educational interventions targeting these populations, applied VR technology integrated with game-based components such as scoring systems, feedback mechanisms, or challenges, and reported at least one quantitative learning outcome (e.g., knowledge, skills, attitudes, or self-efficacy). Only peer-reviewed articles published in academic journals in Korean or English were included. Acceptable study designs were experimental or quasi-experimental studies with control groups. Studies were excluded if they did not involve nursing students or nurses, did not clearly integrate game-based VR elements, or failed to report quantitative learning outcomes. In addition, gray literature such as dissertations, conference abstracts, and non–peer-reviewed reports; single-group designs; qualitative studies; descriptive surveys; meta-analyses; literature reviews; animal experiments; preliminary studies not directly related to the review objectives; and studies without accessible full texts were excluded. A total of 1,072 records were identified through database searches. All records were organized using EndNote X20 and Microsoft Excel 2020 (Microsoft, Redmond, WA, USA). After removing 183 duplicates and excluding 126 gray literature items (e.g., dissertation or conference abstracts), 763 records remained for title and abstract screening. Of these, 634 were excluded for being irrelevant to nursing education or failing to meet inclusion criteria. Subsequently, 129 full-text articles were reviewed, and 105 were excluded for the following reasons: full-text unavailable (n=52), absence of game-based VR intervention (n=28), or lack of quantitative outcome reporting (n=25). Finally, 24 studies met all inclusion criteria and were included in this scoping review (
Figure 1 and
Supplementary Material).
This review was conducted in accordance with the JBI Scoping Review Manual [
22] to systematically map the scope and characteristics of existing research on the topic. Although scoping reviews generally allow for methodological flexibility in study design, the JBI framework permits inclusion or exclusion of specific designs depending on the review’s purpose and research questions. To ensure objective comparison and analysis of learning outcomes in game-based VR educational programs, this review focused exclusively on quantitative comparative studies (experimental or quasi-experimental designs with control groups) that clearly reported intervention effects.
The study selection process followed the procedures of a scoping review, and the flow of study selection was described in accordance with PRISMA-ScR guidelines [
23]. Data extraction was independently conducted by two reviewers—a professor with a PhD in nursing and a PhD candidate in nursing—using a data extraction tool recommended by the JBI methodology [
22]. Extracted data included study characteristics (author, year of publication, and country), study population, study design, details of the game-based VR intervention, and educational outcomes. Any disagreements between reviewers were resolved through discussion and consensus. In addition, a manual search was performed by examining the reference lists of included studies to identify potentially overlooked publications.
The extracted data were categorized and descriptively summarized according to the objectives of the scoping review. Studies with related content were grouped into categories emphasizing the structural characteristics of the interventions (e.g., implementation settings, target population, program components), the design features of the educational programs (e.g., gamification techniques, feedback mechanisms, learning strategies), and the reported effects on learning outcomes (e.g., knowledge, skills, attitudes, self-efficacy). The main features and differences across studies within each category were compared and analyzed to identify overarching trends and recurring patterns in the research.
7. Ethical Considerations
Because this study was a literature review and the researchers had no access to study participants or their personal information, there were no ethical concerns. Accordingly, this study was exempt from review by the Keimyung University Ethics Committee (40525-202403-HR-001-02).
RESULTS
1. General Characteristics
The general characteristics of the 24 studies included in this review are summarized in
Tables 1 and
2.
1) Year of publication
By year of publication, one study (4.2%) was published in each of 2015, 2019, and 2020 [A1-3]. Three studies (12.5%) were published in 2021 [A4-6], six studies (25.0%) in 2022 [A7-12], four studies (16.7%) in 2023 [A13-16], five studies (20.8%) in 2024 [A17-21], and three studies (12.5%) in 2025 [A22-24].
2) Country of study
South Korea accounted for the largest proportion of studies (11 studies, 45.8%) [A5,A6,A8,A11-14,A16,A19,A20,A23]. This was followed by Taiwan with three studies (12.5%) [A3,A9,A21]. One study (4.2%) each was conducted in Portugal [A1], Turkey [A2], Brazil [A4], Cyprus [A7], China [A10], Germany [A15], Hong Kong [A17], Palestine [A18], the United States [A22], and Finland [A24].
3) Study population and sample size
Most studies targeted nursing students, accounting for 21 studies (87.5%) [A1-8,A10-15,A17,A18,A20-24], while three studies (12.5%) targeted practicing nurses [A9,A16,A19]. Sample sizes ranged from 14 to 202 participants. Six studies (25.0%) included fewer than 50 participants [A1,A4,A14,A16,A19,A20], while 10 studies (41.7%) involved 50 to 100 participants [A2,A5,A6,A8,A9,A11,A12,A21,A22,A24]. Five studies (20.8%) included 100 to 150 participants [A3,A7,A13,A15,A18], and three studies (12.5%) had sample sizes of 150 or more [A10,A17,A23].
4) Topics of studies
Among the 24 included studies, the most common topics were infection control and patient safety [A3,A6,A7,A12,A14,A16] and basic nursing skills [A2,A4,A8,A11,A15,A23], each addressed in six studies (25.0%). Four studies (16.7%) focused on geriatric and specialized nursing areas, such as pressure ulcer care, neonatal care, and neurological assessment [A1,A19-21]. Three studies (12.5%) each examined mental health nursing and empathy education [A5,A22,A24] or disaster and emergency response [A9,A10,A17]. Anatomy education was the topic of two studies (8.3%) [A13,A18].
2. Types and Learning Factors of Game-Based VR Programs in Nursing Education
1) Types of programs
Based on technological structure, many of the included programs incorporated multiple technology components, such as HMDs, mobile devices, and web-based platforms, meaning that a single study could fall into more than one category. HMD-based immersive VR programs were the most common, reported in 14 studies (58.3%) [A1,A3,A6,A9-17,A21,A24]. Programs combining multiple technologies—such as HMDs with mobile or web platforms, whether integrated structurally or through content—were found in six studies (25.0%) [A4,A5,A16,A19,A20,A22]. Programs employing web-based or metaverse platforms were reported in four studies (16.7%) [A2,A8,A22,A23], and mobile-based VR programs were used in three studies (12.5%) [A2,A4,A7]. Additionally, simulations using hand-tracking or high-precision interactive technologies appeared in three studies (12.5%) [A12,A15,A24] (
Table 2).
2) Learning factors of the programs
All 24 studies (100%) incorporated designs enabling learners to engage in self-directed learning by repeatedly practicing scenarios without constraints of time or location [A1-24]. Immediate feedback was provided in 22 studies (91.7%) [A1-4,A6-12,A14-24], while interaction-centered learning environments were implemented in 21 studies (87.5%) [A1-3,A5-11,A13-17,A19-24]. Among these, nine studies (37.5%) [A5-7,A12,A16,A17,A19,A23,A24] incorporated debriefing or self-assessment components beyond simple interactions, facilitating learner reflection and deeper understanding (
Table 2).
3) Gamification elements
All 24 studies (100%) integrated at least one gamification element [A1-24]. The most frequent element was scenario-based, stepwise progression, reported in 21 studies (87.5%) [A1-3,A5-11,A13-17,A19-24]. Mission-based task presentation appeared in 20 studies (83.3%) [A1-3,A5-11,A13-17,A19-22,A24]. Retry and feedback structures following errors were included in 19 studies (79.2%) [A1-3,A6-11,A13-17,A19,A21-24]. Emotional immersion features, such as virtual patient responses, were implemented in 19 studies (79.2%) [A1-3,A5-11,A13,A14,A16,A17,A19-22,A24]. Sensory enhancement features, including animation and voice feedback, were found in 17 studies (70.8%) [A1,A2,A5-11,A13,A14,A16,A17,A19,A21,A24]. Finally, structures involving challenge and reward through repetition were incorporated in 17 studies (70.8%) [A1-3,A6-11,A13-17,A19,A21,A24] (
Table 2).
1) Primary outcomes
The primary outcomes measured in the included studies were knowledge acquisition, self-efficacy, skill performance, learning motivation, and engagement. Knowledge acquisition was reported to have improved in 21 studies (87.5%) [A1-3,A5, A7,A8,A10-24] through the application of game-based VR. Enhanced self-efficacy was observed in 20 studies (83.3%) [A1,A3,A5-17,A20-24], while increased learning motivation and engagement were reported in 18 studies (75.0%) [A1,A3,A5-11,A13,A14,A16,A17,A19-22,A24]. Significant improvements in skill performance were identified in 17 studies (75.0%) [A2,A3,A6,A7,A9-14,A16,A17,A19-22,A24], particularly in nursing procedures such as intravenous injection, anatomical understanding, and infection control (
Table 2).
2) Secondary outcomes
Regarding secondary outcomes, learner satisfaction was reported to increase in 21 studies (87.5%) [A1-3,A5-14,A16,A17,A19-24], and an improved sense of immersion was noted in 20 studies (83.3%) [A1-3,A5-14,A16-21,A24]. Enhanced emotional responses, such as greater interest and empathy, were identified in 18 studies (75.0%) [A1,A3,A5-11,A13,A14,A16,A17,A19-22,A24], while improvements in teamwork and communication skills were reported in six studies (25.0%) [A6,A8,A13,A14,A19,A22] (
Table 2).
DISCUSSION
This study conducted a scoping review of intervention studies on game-based VR programs for nursing education published in domestic and international journals, aiming to systematically analyze the characteristics and educational effects of these interventions and to propose future directions. Analysis of 24 intervention studies revealed that game-based VR programs had positive effects on skill performance, knowledge acquisition, self-efficacy, learning motivation, and learner satisfaction. The integration of various learning strategies and gamification elements demonstrated that such programs can be effectively utilized as meaningful instructional approaches in nursing education.
According to research trends, studies applying game-based VR in nursing education began in 2015 and increased sharply following the COVID-19 pandemic. This surge can be attributed to the suspension of clinical practicums and restrictions on face-to-face instruction during the pandemic, which significantly reduced experiential learning opportunities and compelled nursing schools to adopt new instructional modalities, thereby accelerating the demand for non-face-to-face education [
28]. In this context, the need for learner-centered and immersive educational environments intensified, and game-based VR programs gained prominence as practical instructional strategies capable of compensating for limited clinical exposure while fostering higher-order competencies such as problem-solving, critical thinking, and clinical judgment [
29].
The geographical distribution of studies was concentrated in Asian countries, particularly South Korea. East Asian nations have actively promoted the integration of innovative educational technologies into nursing curricula, supported by high levels of acceptance of artificial intelligence technologies and strong technology-oriented policy environments [
30]. Within this framework, the adoption of VR technology as part of simulation-based and personalized learning strategies has expanded rapidly. Eleven of the included studies were conducted in South Korea, representing the largest proportion. This predominance likely reflects not only the relatively high number of VR-related publications in Korean nursing education but also the structural characteristics of nursing programs and the strong policy support for educational technology. In South Korea, nursing education has shown sustained interest in applying information and communication technologies to overcome the limitations of traditional clinical practicums, such as restricted access to clinical sites, patient safety concerns, and ethical issues [
31]. Consequently, many nursing schools have established simulation centers and built VR-based training infrastructure, with digital technologies becoming increasingly embedded in clinical education. These developments have been further facilitated by government support, particularly through initiatives such as the Ministry of Education’s policies, local government programs, and the University Innovation Support Project, which have collectively encouraged research and innovation in this field [
32]. Therefore, the high proportion of Korean studies in this review likely reflects both publication activity and the existence of a well-developed system supporting technology-driven educational innovation in Korean nursing education. Nonetheless, because the studies were concentrated in specific regions, caution is warranted when generalizing these findings to countries or educational settings with different cultural or institutional contexts, as identical VR interventions may yield differing effects elsewhere.
Among the 24 studies reviewed, 20 studies (83.3%) [A1,A2,A4-8,A10-15,A17,A18,A20-24] targeted nursing students, whereas only four (16.7%) [A3,A9,A16,A19] involved clinical nurses. Studies focusing on nursing students primarily addressed foundational competencies such as basic nursing skills, infection control, anatomy, and mental health nursing, with outcomes emphasizing knowledge acquisition, skill performance, learning motivation, and self-efficacy. In contrast, studies involving nurses addressed patient safety-related topics in clinical practice, including neonatal intensive care unit infection control, disaster response, and pressure ulcer management. These studies predominantly reported outcomes concerning clinical applicability, such as situational response ability, clinical judgment, self-efficacy, and confidence in infection control performance. These findings suggest that for nursing students, VR serves as a means to develop essential competencies and facilitate transition to clinical practice, whereas for nurses, it functions as an advanced learning tool to enhance patient safety and professional decision-making. Accordingly, future research should differentiate between these two learner populations, comparing and analyzing their educational characteristics and learning outcomes to establish optimized VR instructional strategies tailored to each group. Moreover, the included studies generally employed small to moderate sample sizes, with most involving fewer than 100 participants, reflecting the exploratory stage of current research and resource limitations. Future investigations should broaden participant inclusion to encompass new graduates and nurses with experience in diverse clinical settings. Employing more segmented research designs that account for variables such as specialty area and technological acceptance level will be essential for validating the practical applicability and educational utility of game-based VR interventions. In terms of topic distribution, game-based VR programs were applied across a range of nursing education domains, including infection control and patient safety, basic nursing skills, mental health nursing, disaster nursing, geriatric nursing, and specialized nursing fields. Among these, infection control and basic nursing skills were the most frequently addressed topics, reflecting the current emphasis in nursing education on patient safety and the acquisition of core clinical competencies [
33]. However, studies focusing on complex nursing situations requiring higher-order reasoning—such as team-based care, community health nursing, and clinical decision-making—remain limited. Future research should extend beyond narrowly defined, procedure-oriented topics to encompass integrated nursing scenarios that mirror the complexity of real-world practice and promote the development of interdisciplinary collaboration skills.
In terms of the technological characteristics of intervention designs, most studies employed immersive VR HMDs. These devices effectively supplemented limited clinical training environments by enabling learners to repeatedly engage in clinical scenarios without physical or temporal constraints. Furthermore, follow-up learning structures incorporating debriefing, reflective questioning, and self-assessment were found to enhance learners’ self-directedness and reflective capacity. Feedback was included in nearly all interventions; immediate and specific feedback was effective in promoting error recognition and self-correction among learners [
10,
12]. This finding suggests that prompting learners to identify and correct their own mistakes during performance plays a crucial role in strengthening both skill acquisition and critical thinking abilities [
34].
All intervention programs incorporated at least one gamification element to promote learner engagement and immersion. In particular, scenario-based stepwise progression [A1-3,A5-11,A13-17,A19-24], mission-style task structures [A1-3,A5-11,A13-17,A19-22,A24], immediate retry and feedback mechanisms following errors [A1-3,A6-11,A13-17,A19,A21-24], and emotional responses from virtual patients [A1-3,A5-11,A13,A14,A16,A17,A19-22,A24] were central design strategies used to encourage repeated practice and active cognitive engagement in realistic clinical contexts. According to gamification theory, challenge-and-reward-based structures enhance learners’ self-efficacy and motivation for continued learning [
13]. In medical education, repeated task execution combined with immediate feedback has also been shown to be an effective strategy for fostering immersion and improving technical proficiency [
14]. Ultimately, gamification elements extend beyond merely stimulating interest—they create a learning environment that sustains both cognitive engagement and emotional immersion. These results indicate that gamification can serve as an effective pedagogical strategy for strengthening clinical judgment and problem-solving abilities in nursing education.
Regarding program effectiveness, the included studies consistently demonstrated positive changes across multiple learning outcomes, including knowledge acquisition, self-efficacy, learning motivation, and skill performance. Knowledge acquisition improved in nearly all studies, suggesting that VR-based learning effectively enhances understanding and retention by presenting scenarios that closely mirror real clinical environments [
10]. The consistent improvement in self-efficacy across studies indicates that immersive environments, repeated practice, and immediate feedback collectively contribute to developing learners’ confidence and self-directedness. Design features such as gamification components, audiovisual stimulation, and progressive challenges played a significant role in maintaining learning motivation and engagement by eliciting emotional responses and supporting sustained participation [A1-24]. In terms of skill performance, several studies reported that VR-based simulation training enhanced practical nursing skills, including intravenous injection, anatomical knowledge, and infection control [A3,A7,A12,A16,A18,A23]. These findings suggest that VR education contributes not only to theoretical knowledge but also to the development of practical competencies. However, current VR interventions may not fully capture the complexity and unpredictability of real clinical settings. Therefore, future interventions should incorporate more realistic, integrated clinical contexts to enhance practical relevance and transferability.
In addition to cognitive and technical outcomes, most studies reported high levels of learner satisfaction and engagement [A1-3,A5-11,A13,A14,A16,A17,A19-24], along with positive emotional responses such as interest and empathy [A1,A3,A5-11,A13,A14,A16,A17,A19-22,A24]. These results suggest that gamified VR environments effectively foster emotional immersion, transforming the learning process into a more enjoyable and meaningful experience [
35]. However, improvements in teamwork and communication skills were reported in only a few studies [A6,A8,A13,A14,A19,A22], likely because most interventions emphasized individual learning rather than collaborative engagement. Consequently, future studies should incorporate collaborative learning frameworks that promote interactive, team-based competencies reflective of real clinical practice.
This study aimed to analyze the impact of game-based VR programs on nursing education from multiple perspectives. Whereas previous research has tended to focus on discrete outcome measures emphasizing educational effectiveness, this study is significant in that it provides a descriptive analysis of both the design components—such as technological implementation, gamification structure, feedback mechanisms, and reflective learning frameworks—and the learning outcomes. By examining not only the educational content but also the delivery modes and structural elements of learning, this study offers practical insights and strategic directions for the design and implementation of future educational programs.
However, this study had several limitations. Most of the included studies targeted nursing students; therefore, it remains uncertain whether similar effects can be expected among nurses actively working in clinical settings. In addition, many studies employed relatively small sample sizes, necessitating cautious interpretation of the results. A considerable proportion of the studies were also conducted within specific regions, particularly South Korea, which may limit the generalizability of the findings to countries or educational environments with different cultural and institutional contexts. Future research should therefore include diverse learner populations, evaluate the sustainability of intervention effects and their applicability in clinical practice, and conduct multicultural comparative studies across different national and educational settings. Nevertheless, this review excluded qualitative studies, single-group designs, and gray literature, which may restrict the comprehensiveness typically expected of scoping reviews. These exclusions could increase the potential for publication, design, or language bias. Future reviews should consider incorporating more diverse study designs and data sources to capture contextual factors, learner experiences, and implementation processes that may not be adequately reflected in quantitative evidence alone.
Building upon these findings and limitations, the implications for practice and research are that, when designing game-based VR programs, instructors should carefully structure the learning experience to align meaningfully with educational goals and avoid restricting the design to technical implementation alone. Feedback mechanisms, repeated practice, and strategies to promote immersion should be developed within a pedagogical framework that comprehensively considers learner characteristics, instructional objectives, and implementation methods. Moreover, content accessibility and ease of technology use are essential factors for establishing effective educational strategies.
CONCLUSION
This scoping review found that game-based VR programs demonstrated positive educational effects across multiple aspects of nursing education, including improvements in learners’ knowledge, skill performance, self-efficacy, learning motivation, emotional engagement, and learning satisfaction. In particular, immersive and repeatable learning environments, immediate feedback, and gamified challenge-based elements were effective in promoting active participation and self-directed learning. However, most studies were limited to nursing students, and evidence regarding the applicability of these interventions in real clinical settings and their long-term effects remains insufficient. Furthermore, the effectiveness of game-based VR programs in enhancing social competencies, such as teamwork and communication skills, was verified in only a few studies, likely due to the predominance of individually structured learning formats. Future research should therefore include diverse learner groups and incorporate real-world clinical contexts to establish the broader educational and practical utility of game-based VR programs in nursing.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and design - MP and KJM; data acquisition and analysis - MP and KJM; interpretation of the findings - MP and KJM; and drafting and critical revision of the manuscript for important intellectual content - MP and KJM.
-
FUNDING
None.
-
ACKNOWLEDGEMENT
None.
-
DATA AVAILABILITY STATEMENT
No new data were created or analyzed during this study. Data sharing is not applicable to this article.
SUPPLEMENTARY MATERIAL
Figure 1.Flow diagram of literature selection. VR=virtual reality.
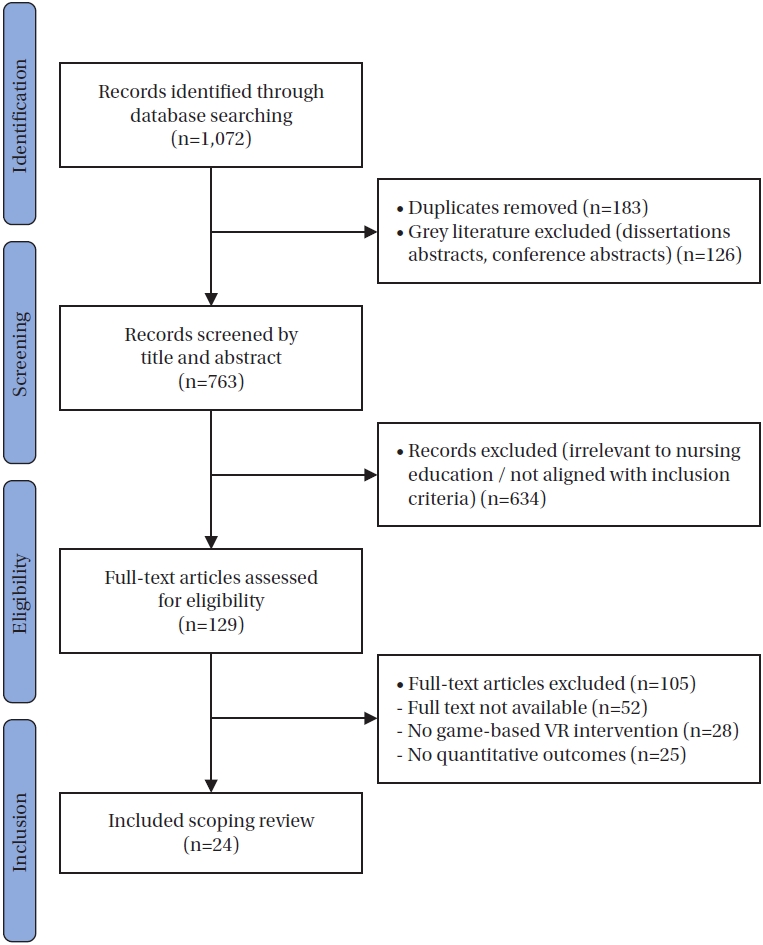
Table 1.Characteristics of Included Literature (N=24)
|
Variables |
Categories |
n (%) |
|
Publication year |
2015 |
1 (4.2) |
|
2019 |
1 (4.2) |
|
2020 |
1 (4.2) |
|
2021 |
3 (12.5) |
|
2022 |
6 (25.0) |
|
2023 |
4 (16.7) |
|
2024 |
5 (20.8) |
|
2025 |
3 (12.5) |
|
Country |
South Korea |
11 (45.8) |
|
Taiwan |
3 (12.5) |
|
Brazil |
1 (4.2) |
|
China |
1 (4.2) |
|
Cyprus |
1 (4.2) |
|
Finland |
1 (4.2) |
|
Germany |
1 (4.2) |
|
Hong Kong |
1 (4.2) |
|
Palestine |
1 (4.2) |
|
Portugal |
1 (4.2) |
|
Turkey |
1 (4.2) |
|
USA |
1 (4.2) |
|
Participants |
Nursing students |
21 (87.5) |
|
Nurses |
3 (12.5) |
|
Sample size |
<50 |
6 (25.0) |
|
≥50 to <100 |
10 (41.7) |
|
≥100 to <150 |
5 (20.8) |
|
≥150 |
3 (12.5) |
|
Topic classification |
Infection control, patient safety |
6 (25.0) |
|
Fundamental nursing skills |
6 (25.0) |
|
Geriatric and specialized nursing areas (e.g., pressure ulcer care, neonatal nursing, neurological assessment) |
4 (16.7) |
|
Psychiatric nursing, empathy education |
3 (12.5) |
|
Disaster, emergency response |
3 (12.5) |
|
Anatomy education |
2 (8.3) |
Table 2.Characteristics of the Included Studies
|
Author (year) |
Country |
Participants |
Topic area |
Type of program |
Learning factors |
Gamification elements |
Primary outcomes |
Secondary outcomes |
Reference no. |
|
Fonseca et al. (2015) |
Portugal |
14 nursing students |
Preterm newborn clinical assessment/neonatal nursing |
Web-based serious game (e-Baby) |
Autonomy, interactivity, feedback, self-directed learning |
Scenario-based simulation, virtual patient, decision-making, feedback |
Increased knowledge and clinical reasoning on oxygenation assessment |
High learner satisfaction, motivation, usability, engagement |
A1 |
|
Biyik Bayram and Caliskan (2019) |
Turkey |
86 nursing students (1st year) |
Tracheostomy care |
Game-based VR mobile phone application |
Repetition, feedback, self-directed learning, skill acquisition, theoretical-practical integration |
Game scenario, character-based simulation, stage-based tasks, mobile-based access, performance feedback |
Experimental group showed significantly higher skill performance in tracheostomy suction and skin care |
Higher motivation, better engagement, potential for independent and repeated practice anytime/anywhere |
A2 |
|
Wu et al. (2020) |
Taiwan |
109 (59 nurses, 50 medical interns) |
Needle stick/sharp injury prevention |
VR-based training using Gagne’s model |
Familiarity, confidence, knowledge retention, reduction of anxiety, engagement, instructional design alignment |
Random scenarios, decision-based tasks, feedback loops, immersive gameplay, performance tracking |
Increased familiarity and confidence with universal precautions, improved performance after VR training, and reduced needle stick injury rates |
Decreased anxiety, improved speed and accuracy in decision tasks, better retention of learning effects over 2 months |
A3 |
|
Girao et al. (2021) |
Brazil |
14 nursing students (usability test), 8 faculty evaluators |
Medication preparation and administration |
Serious game-based VR simulation |
Motivation, immersion, satisfaction, learning, decision-making, cognitive engagement |
Interactive VR environment, simulated patient, hand hygiene quiz, color-coded meds, end of task feedback |
High usability ratings (100% in immersion, satisfaction, and learning); validated as “very good” by experts |
Positive influence on short and long-term learning, high user engagement, practical skill reinforcement |
A4 |
|
Lee et al. (2021) |
South Korea |
70 nursing students (4th year; Exp. 35, Cont. 35) |
Psychiatric nursing practice |
Case-based VR simulation |
Knowledge, learning self-efficacy, problem-solving ability |
Repetition, feedback, stage lock, animation based interaction |
Improved psychiatric nursing knowledge, learning self-efficacy, and problem-solving ability |
Partial improvement in therapeutic communication and communication confidence; no difference in learning immersion |
A5 |
|
Yu et al. (2021) |
South Korea |
50 nursing students (4th year; Exp. 25, Cont. 25) |
High-risk neonatal infection control |
VR simulation using HMD+leap motion (HirNIC VR) |
Prebriefing, debriefing, scenario-based simulation, NLN/Jeffries Framework |
Immersive VR, scenario-driven simulation, hand-tracking |
Performance self-efficacy, learner satisfaction |
Knowledge (no significant change) |
A6 |
|
Al Mugheed et al. (2022) |
Cyprus |
126 nursing students (3rd & 4th year) |
Standard precautions education |
Game-based VR phone application+online education |
Self-paced learning, team-based lab practice, quizzes, recorded lessons, repeatable playback |
Game scenarios, interactive VR phone application |
Knowledge, attitude, compliance with standard precautions |
None |
A7 |
|
An (2022) |
South Korea |
72 nursing students (2nd year; Exp. 34, Cont. 38) |
Core nursing skills: vital signs & subcutaneous injection |
Metaverse-based simulation |
ASSURE model-based design, repeated individual scenario learning, pre, post debriefing |
Interactive scenario, 3D virtual world, object selection, embedded quiz |
Knowledge, Performance confidence, clinical competency (all improved) |
None |
A8 |
|
Chang et al. (2022) |
Taiwan |
67 ER nurses (Exp. 32, Cont. 35) |
Chemical disaster preparedness |
360° VR-based simulation vs. tabletop drill |
Role-playing (incident commander, triage, decontamination), H.A.Z.M.A.T. protocol, adaptive quiz, feedback loop (video rewatch for incorrect answers) |
Immersive VR, scenario-based triage, MCQ with instant feedback, embedded learning videos, first-person experience |
Self-preparedness, Self-efficacy (short-term improvement) |
No sustained difference at 3-week follow-up |
A9 |
|
Hu et al. (2022) |
China |
158 nursing students (Exp. 78, Cont. 80) |
Disaster evacuation management |
VR-based mobile game application vs. traditional lecture |
Scenario-based VR learning (fire, earthquake, CPR), repeated testing, feedback, mobile accessibility, self-directed |
Interactive disaster scenario game, scoring system, real-time physiological response |
Knowledge retention, decision-making ability, instructional satisfaction |
None |
A10 |
|
Yang and Oh (2022) |
South Korea |
83 nursing students (VR 29, Simulation 28, Cont. 26) |
Neonatal resuscitation education |
Immersive VR gamification program (based on Keller’s ARCS model) vs. high-fidelity simulation vs. online lecture |
ARCS model including perceptual arousal, goal orientation, motive matching, learning requirements |
Scenario-based challenges, immediate feedback, repetition on failure, immersive VR environment, reward system |
Improvement in neonatal resuscitation knowledge, problem-solving ability, self-confidence, and learning motivation |
Reduction in anxiety (notably in simulation group), improvement in clinical reasoning (no significant group difference) |
A11 |
|
Yu and Yang (2022) |
South Korea |
50 nursing students (3rd and 4th year, Exp. 25, Cont. 25) |
Infection control and respiratory care for pediatric COVID-19 patients |
VRICS program with prebriefing, simulation, debriefing |
Based on self-efficacy theory; PPE knowledge, infection control performance, confidence, and immersion |
Scenario-based VR with HMD, structured steps, real-time interaction and feedback |
Improved PPE knowledge, infection control performance, and self-efficacy in the experimental group compared to control group |
High levels of realism and learner satisfaction |
A12 |
|
Kim et al. (2023) |
South Korea |
113 nursing students (1st year, Exp. 56, Cont. 57) |
Anatomy education using VR |
VR-based anatomy education vs. anatomage table (3D dissection table) |
Learning presence, technology acceptance, learning motivation, anatomy knowledge (based on ARCS and TAM frameworks) |
Interactive 3D organ modeling via Oculus (3D Organon VR Anatomy), real-time manipulation (rotate, zoom, dissect) |
Increased learning presence, higher technology acceptance, and improved anatomy knowledge in the VR group |
No significant difference in learning motivation between groups |
A13 |
|
Oh and Kim (2023) |
South Korea |
44 nursing students (3rd year, Exp. 22, Cont. 22) |
Patient safety management education |
VR-based smartphone application program focusing on clinical safety (patient ID, infection control, medication) |
Knowledge, attitude, and confidence in patient safety (based on self-efficacy and experiential learning principles) |
VR headset (Oculus Quest 2), scenario-based learning, mobile accessibility, interactive tasks, feedback |
Improvement in patient safety knowledge, attitudes, and performance confidence in the experimental group |
High engagement and usefulness as preclinical orientation material |
A14 |
|
Plotzky et al. (2023) |
Germany |
131 nursing students (2nd, 3rd year, VR high 47, VR low 41, video 43) |
Endotracheal suctioning skill training |
Two types of immersive VR simulations (high-tech & low-tech) vs. instructional video |
Knowledge, skill performance, learning satisfaction, technology acceptance (TAM-based: usefulness, ease of use) |
VR simulation with scenario-based steps, real-time feedback, hand-tracking (VR high), gamified errors (e.g., germs shown) |
Knowledge significantly improved in all groups (no difference between groups); skill performance best in video group |
Higher learner satisfaction in VR low group; technology acceptance higher in VR low than VR high group |
A15 |
|
Ryu and Yu (2023) |
South Korea |
40 NICU nurses (Exp. 20, Cont. 20) |
Advanced infection control in NICU |
VR simulation program for preventing central line-associated bloodstream infections and ventilator-associated pneumonia (VR_AICENICU) |
Infection control knowledge, performance confidence, presence, empathy, program satisfaction |
Scenario-based VR with HMD, hand-tracking, immersive audio, progression-based simulation steps |
Improved infection control confidence in the experimental group basic infection control knowledge significantly improved |
The experimental group reported high levels of presence, empathy, and satisfaction |
A16 |
|
Chan et al. (2024) |
Hong Kong |
202 undergraduate nursing students (preclinical, VR-Hospital exposure) |
Development of nontechnical skills |
Immersive VR training using VR-Hospital (multi-bed, multi-patient, multi-task single-user game) |
Situation awareness, communication, teamwork, leadership, decision-making, satisfaction, self-confidence, sense of presence |
Scenario-based multi-task virtual ward, voice interaction, real-time decision-making, randomized events, reflection via MCQs |
Improvement in nontechnical skills (communication, teamwork, decision-making), self-confidence, and satisfaction |
High sense of presence and realism (physical, psychological, affective fidelity) students experienced stress and multitasking |
A17 |
|
Jallad et al. (2024) |
Palestine |
138 year nursing students (1st year single group, pre-post-test) |
Anatomy education (musculoskeletal system) |
Immersive VR application for human anatomy course using Meta Quest 2 (before and after musculoskeletal lecture) |
Technology acceptance model; ease of use, interaction, imagination, immersion, motivation, intention to use |
Interactive 3D human anatomy visuals, spatial navigation, real-time engagement, high-fidelity simulation (Meta Quest 2) |
Increased student satisfaction, improved anatomy knowledge, and positive perceptions toward immersive VR after the lecture |
High levels of motivation, immersion, and intention to continue using VR for learning |
A18 |
|
Jung and Moon (2024) |
South Korea |
35 novice nurses (<2 years’ experience, Exp. 18, Cont. 17) |
Pressure ulcer prevention and management |
VR simulation program (PU-VRSim) based on Kolb’s experiential learning theory and ADDIE model |
Pressure ulcer knowledge, clinical judgment, self-efficacy, critical thinking |
Scenario-based simulation, real-time interaction via HMD and controller, patient case progression, feedback, immersive visuals |
Improved pressure ulcer knowledge in both groups; accomplished level of clinical judgment in VR group |
Positive learning experience (realism, engagement, usability); some equipment-related discomfort reported |
A19 |
|
Kim et al. (2024) |
South Korea |
49 nursing students (4th year, one-group pre-post test) |
Nervous system assessment in clinical education |
Virtual game-based integrated clinical practice simulation program (nervous system assessment) |
Self-directed learning, academic self-efficacy, learning presence, learning flow (based on Kolb’s experiential learning theory) |
Scenario-based VR simulation, role-play, interactive assessments (GCS, motor, pupil), feedback, repeated practice |
Significant improvement in self-directed learning and learning presence |
No significant change in academic self-efficacy and learning flow students reported high engagement and realism |
A20 |
|
Lin et al. (2024) |
Taiwan |
50 nursing students (1st-3rd year, Exp. 25, Cont. 25) |
Geriatric oral health care |
Virtual reality-based oral health simulation (2 sessions over 4 weeks) |
Knowledge, attitude, self-efficacy, behavioral intention (based on experiential learning theory) |
Scenario-based VR training, 3D interactive tasks with feedback, repeated trial, HMD use with motion sensors |
Significant improvement in knowledge, attitude, self-efficacy, and behavioral intention in the experimental group |
High satisfaction with VR system, supports integrating VR in nursing curriculum |
A21 |
|
Huang et al. (2025) |
United States |
69 nursing students (2nd-4th year, randomly assigned to 4 groups) |
Affective empathy development via VR |
2×2 factorial design: VR vs. non-VR×clinician vs. parent perspective, using the game That Dragon, Cancer |
Perceived self-location, narrative transportation, emotional engagement, affective empathy (based on empathy theory) |
Immersive storytelling, first person narrative, emotional role-play, interaction with characters (Oculus Go, 360° view) |
VR improved sense of presence (self-location) clinician perspective increased emotional engagement |
Affective empathy increased through a mediated pathway (self-location → transportation → emotional engagement → empathy) |
A22 |
|
Kim and Lee (2025) |
South Korea |
184 nursing students (2nd year, Exp. 92, Cont. 92) |
Intravenous injection training |
Web-based VR intravenous injection program (real video, speech interaction, no HMD required) |
Knowledge, confidence, satisfaction (based on experiential and self-directed learning) |
Real-scenario videos, branching dialogues, interactive learning via voice commands (mobile/PC accessible) |
Improved knowledge and confidence in IV injection in the experimental group |
Higher satisfaction with clinical training in the experimental group |
A23 |
|
Koivisto et al. (2025) |
Finland |
52 graduating nursing students (from 3 universities of applied sciences) |
Empathy development in nursing |
Immersive VR simulation game using Oculus Quest HMD and hand controllers (first-person nurse role scenario) |
Empathic concern, cognitive empathy, helping motivation, shared affect, distress, empathic imagination |
Scenario-based patient care, clinical assessment (ABCDE), multisensory feedback, voice/hand interaction, immersive navigation |
Positive experience of empathy (especially helping motivation and concern); positive user experience in all dimensions |
Younger students reported more distress; older students showed greater cognitive empathy; prior work experience enhanced shared emotional understanding |
A24 |
REFERENCES
- 1. Catton H. Nursing in the COVID-19 pandemic and beyond: protecting, saving, supporting and honouring nurses. Int Nurs Rev. 2020;67(2):157-9. https://doi.org/10.1111/inr.12593
- 2. World Health Organization (WHO). Nursing and midwifery [Internet]. Geneva: WHO; 2020 [cited 2025 June 24]. Available from: https://www.who.int/news-room/fact-sheets/detail/nursing-and-midwifery
- 3. Taylor DC, Hamdy H. Adult learning theories: implications for learning and teaching in medical education: AMEE Guide No. 83. Med Teach. 2013;35(11):e1561-72. https://doi.org/10.3109/0142159x.2013.828153
- 4. Hatlevik IK. Meaningful connections: A study of connections between learning in various arenas and the development of different aspects of professional competence among students in nursing, teacher, and social work education. Oslo: Høgskolen i Oslo og Akershus; 2014.
- 5. European Association for Quality Assurance in Higher Education (ENQA); European Students’ Union (ESU); European University Association (EUA); European Association of Institutions in Higher Education (EURASHE). Standards and guidelines for quality assurance in the European Higher Education Area (ESG). Brussels: ENQA; 2015.
- 6. Bradley CS, Johnson BK, Dreifuerst KT. Debriefing: a place for enthusiastic teaching and learning at a distance. Clin Simul Nurs. 2020;49:16-8. https://doi.org/10.1016/j.ecns.2020.04.001
- 7. Liu K, Zhang W, Li W, Wang T, Zheng Y. Effectiveness of virtual reality in nursing education: a systematic review and meta-analysis. BMC Med Educ. 2023;23(1):710. https://doi.org/10.1186/s12909-023-04662-x
- 8. Mendez KJ, Piasecki RJ, Hudson K, Renda S, Mollenkopf N, Nettles BS, et al. Virtual and augmented reality: implications for the future of nursing education. Nurse Educ Today. 2020;93:104531. https://doi.org/10.1016/j.nedt.2020.104531
- 9. Weiner E, Gordon J, Rudy S, McNew R. Expanding virtual reality to teach ultrasound skills to nurse practitioner students. Stud Health Technol Inform. 2019;264:893-7. https://doi.org/10.3233/shti190352
- 10. Foronda CL, Fernandez-Burgos M, Nadeau C, Kelley CN, Henry MN. Virtual simulation in nursing education: a systematic review spanning 1996 to 2018. Simul Healthc. 2020;15(1):46-54. https://doi.org/10.1097/sih.0000000000000411
- 11. Plotzky C, Lindwedel U, Sorber M, Loessl B, Konig P, Kunze C, et al. Virtual reality simulations in nurse education: a systematic mapping review. Nurse Educ Today. 2021;101:104868. https://doi.org/10.1016/j.nedt.2021.104868
- 12. Zhong Y, Champion JD. Assessing the effectiveness of nursing virtual reality simulation for English as second language students to decrease anxiety in clinical courses. J Nurs Educ Pract. 2024;15(2):46-56.
- 13. Deterding S, Dixon D, Khaled R, Nacke L. From game design elements to gamefulness: defining "gamification". Paper presented at: Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments; 2011, September 28-30; Tampere, Finland. Association for Computing Machinery; 2011. p. 9-15.
- 14. van Gaalen AE, Brouwer J, Schönrock-Adema J, Bouwkamp-Timmer T, Jaarsma AD, Georgiadis JR. Gamification of health professions education: a systematic review. Adv Health Sci Educ Theory Pract. 2021;26(2):683-711. https://doi.org/10.1007/s10459-020-10000-3
- 15. Tavares N. The use and impact of game-based learning on the learning experience and knowledge retention of nursing undergraduate students: a systematic literature review. Nurse Educ Today. 2022;117:105484. https://doi.org/10.1016/j.nedt.2022.105484
- 16. Chen FQ, Leng YF, Ge JF, Wang DW, Li C, Chen B, et al. Effectiveness of virtual reality in nursing education: meta-analysis. J Med Internet Res. 2020;22(9):e18290. https://doi.org/10.2196/18290
- 17. Fathi Najafi T, Andaroon N, Bolghanabadi N, Sharifi N, Dashti S. Gamification in midwifery education: a systematic review. BMC Med Educ. 2025;25(1):297. https://doi.org/10.1186/s12909-025-06880-x
- 18. Kim SK, Eom MR, Park MH. Effects of nursing education using virtual reality: a systematic review. J Korea Contents Assoc. 2019;19(2):661-70. https://doi.org/10.5392/JKCA.2019.19.02.661
- 19. Ahn JW. Factor influencing learning outcome in nursing education using gamification: a scoping review. J Korean Acad Fundam Nurs. 2021;28(4):440-57. https://doi.org/10.7739/jkafn.2021.28.4.440
- 20. Colquhoun HL, Levac D, O'Brien KK, Straus S, Tricco AC, Perrier L, et al. Scoping reviews: time for clarity in definition, methods, and reporting. J Clin Epidemiol. 2014;67(12):1291-4. https://doi.org/10.1016/j.jclinepi.2014.03.013
- 21. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19-32. https://doi.org/10.1080/1364557032000119616
- 22. Peters MD, Marnie C, Tricco AC, Pollock D, Munn Z, Alexander L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119-26. https://doi.org/10.11124/jbies-20-00167
- 23. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467-73. https://doi.org/10.7326/m18-0850
- 24. Jensen L, Konradsen F. A review of the use of virtual reality head-mounted displays in education and training. Educ Inf Technol. 2018;23(4):1515-29. https://doi.org/10.1007/s10639-017-9676-0
- 25. Hodgson E, Bachmann ER, Vincent D, Zmuda M, Waller D, Calusdian J. WeaVR: a self-contained and wearable immersive virtual environment simulation system. Behav Res Methods. 2015;47(1):296-307. https://doi.org/10.3758/s13428-014-0463-1
- 26. Radianti J, Majchrzak TA, Fromm J, Wohlgenannt I. A systematic review of immersive virtual reality applications for higher education: design elements, lessons learned, and research agenda. Comput Educ. 2020;147:103778. https://doi.org/10.1016/j.compedu.2019.103778
- 27. Hamilton D, McKechnie J, Edgerton E, Wilson C. Immersive virtual reality as a pedagogical tool in education: a systematic literature review of quantitative learning outcomes and experimental design. J Comput Educ. 2021;8(1):1-32. https://doi.org/10.1007/s40692-020-00169-2
- 28. Tomietto M, Comparcini D, Simonetti V, Cicolini G. Nursing education: challenges and perspectives in a COVID-19 age. Prof Inferm. 2020;73(3):131-2. https://doi.org/10.7429/pi.2020.733131
- 29. Ordu Y, Calişkan N. Experiences of nurse educators using virtual games in nursing education: a qualitative study. J Nurs Res. 2025;33(1):e368. https://doi.org/10.1097/jnr.0000000000000651
- 30. Lukkahatai N, Han G. Perspectives on artificial intelligence in nursing in Asia. Asian Pac Isl Nurs J. 2024;8:e55321. https://doi.org/10.2196/55321
- 31. Choi GW, Woo M, Ryu A, Kim J. The effectiveness of nursing education using immersive virtual reality or augmented reality: systematic review and meta-analysis. J Korean Acad Soc Nurs Educ. 2024;30(3):197-211. https://doi.org/10.5977/jkasne.2024.30.3.197
- 32. Ministry of Health and Welfare. Call for applications: 2025 Nursing College Clinical Practice Education Support Program [Internet]. Sejong: Ministry of Health and Welfare; 2025 [cited 2025 June 25]. Available from: https://www.mohw.go.kr/board.es?act=view&bid=0003&list_no=1484891&mid=a10501010000
- 33. World Health Organization (WHO). Patient safety curriculum guide: multi-professional edition [Internet]. Geneva: WHO; 2011 [cited 2025 June 28]. Available from: https://www.who.int/publications/i/item/9789241501958
- 34. van de Ridder JM, McGaghie WC, Stokking KM, ten Cate OT. Variables that affect the process and outcome of feedback, relevant for medical training: a meta-review. Med Educ. 2015;49(7):658-73. https://doi.org/10.1111/medu.12744
- 35. Slater M, Sanchez-Vives MV. Enhancing our lives with immersive virtual reality. Front Robot AI. 2016;3:74. https://doi.org/10.3389/frobt.2016.00074
Figure & Data
Citations
Citations to this article as recorded by

- Design and usability of an immersive virtual reality simulation in orthopaedic nursing education: A pilot study
Carla Sílvia Fernandes, Ana Galvão, Cris Renata Grou Volpe, Marta Campos Ferreira
International Journal of Orthopaedic and Trauma Nursing.2026; 61: 101286. CrossRef


 E-SUBMISSION
E-SUBMISSION
