Abstract
-
Purpose
Person-centered care emphasizes the therapeutic relationship between medical staff and patients, founded on mutual trust and understanding. In intensive care settings, there is growing recognition of the need to improve the care environment and promote patient-focused nursing. This study aimed to construct and validate a predictive model explaining person-centered care in intensive care units.
-
Methods
This study employed a cross-sectional design involving 230 intensive care unit nurses working in a tertiary hospital, each with more than one year of direct patient care experience. Data were collected online between March 2 and March 30, 2023. Data analysis was conducted using IBM SPSS ver. 26.0 and AMOS ver. 25.0.
-
Results
Statistically significant pathways were identified from nursing competency to the nursing work environment and person-centered care; from communication competence to teamwork and person-centered care; from nursing professionalism to teamwork and the nursing work environment; and from the nursing work environment to person-centered care. Nursing professionalism indirectly influenced person-centered care through teamwork and the nursing work environment.
-
Conclusion
Enhancing person-centered care in intensive care units requires recognizing the critical roles of communication competence, nursing competency, and the nursing work environment. Developing and implementing educational programs that strengthen communication and nursing competencies, alongside initiatives that improve the nursing work environment, are essential.
-
Key Words: Intensive care units; Person-centered care; Structural equation modeling
INTRODUCTION
Intensive care units (ICUs) provide specialized treatment using life-support devices and continuous monitoring to care for critically ill patients [
1]. Because of the high severity of illness and the complexity of tasks, ICUs primarily deliver disease-centered treatment, requiring exceptional focus and professional expertise [
2]. Intensive care nurses possess specialized knowledge for managing critically ill patients and must demonstrate advanced critical care nursing skills [
3]. These nurses experience substantial physical and psychological stress while caring for severely ill patients due to their heavy workload, uncertain patient prognoses, operation of complex medical equipment, and the responsibility of communicating with families [
4]. Excessive workload and stress can compromise patient safety [
5].
Recently, awareness has increased regarding the importance of patient participation in treatment decision-making [
6]. The medical paradigm has shifted from staff-centered to patient-centered and from disease-oriented to symptom-focused care [
7]. Person-centered care (PCC) involves building therapeutic relationships between healthcare professionals and patients based on mutual trust and understanding [
8]. Nurses who respect patients’ values and autonomy deliver professional care by focusing on individuals and communicating effectively [
9].
PCC and patient-centered care share core elements, including empathy, respect, engagement, relationship communication, shared decision-making, holistic focus, individualized attention, and coordinated care. However, they differ in their ultimate goals. Patient-centered care primarily aims for symptom relief and functional recovery, whereas PCC emphasizes holistic well-being and meaningful living by reflecting the individual’s values and life context. PCC thus represents a broader concept, extending beyond the patient to encompass the person as a whole [
10]. Currently, PCC serves as an overarching concept, reflecting the principle that individualized nursing should be provided to all individuals, regardless of setting or clinical context [
11]. In ICUs, PCC requires that professional nurses with specialized expertise respect and empathize with patients while delivering individualized interventions [
12]. PCC has been shown to reduce hospitalization length and outpatient visits, generate economic benefits through decreased medical costs [
13], and improve patient satisfaction by enhancing nursing service quality [
14]. However, ICU nurses often face challenges implementing PCC due to the urgent nature of tasks, time constraints, and the presence of complex medical equipment that limits interaction [
3,
15]. Therefore, improving the ICU care environment and emphasizing PCC are essential [
16]. Nursing care that respects, empathizes with, and acknowledges patient individuality should be prioritized, and ICU nursing should focus on person-centered holistic care that incorporates patients’ values and preferences [
14].
Numerous studies have examined PCC. The theory of PCC was developed through research identifying four core elements using the person-centered nursing conceptual framework, which has been widely applied to practice and comprehensively articulates the essential components of PCC [
8,
17]. Previous studies have analyzed the defining attributes of PCC in ICUs [
12], examined its practical application [
18], and developed measurement tools [
19]. More recently, research has explored changes in the medical environment and factors influencing PCC during the coronavirus disease 2019 (COVID-19) pandemic [
20,
21]. Structural equation modeling (SEM) has also been used to comprehensively examine PCC among nurses [
22,
23]. However, most previous studies have focused on diverse clinical settings such as general wards, limiting their applicability to the unique environment and structural demands of ICUs. Although some studies included ICU nurses as participants, few have conducted an in-depth investigation of how PCC is implemented in ICUs, where continuous monitoring, specialized treatment, and rapid responses to critical events are prioritized. Accordingly, the present study aims to elucidate the factors influencing PCC in the specialized ICU context, providing an empirical foundation for improving the quality of ICU nursing practice.
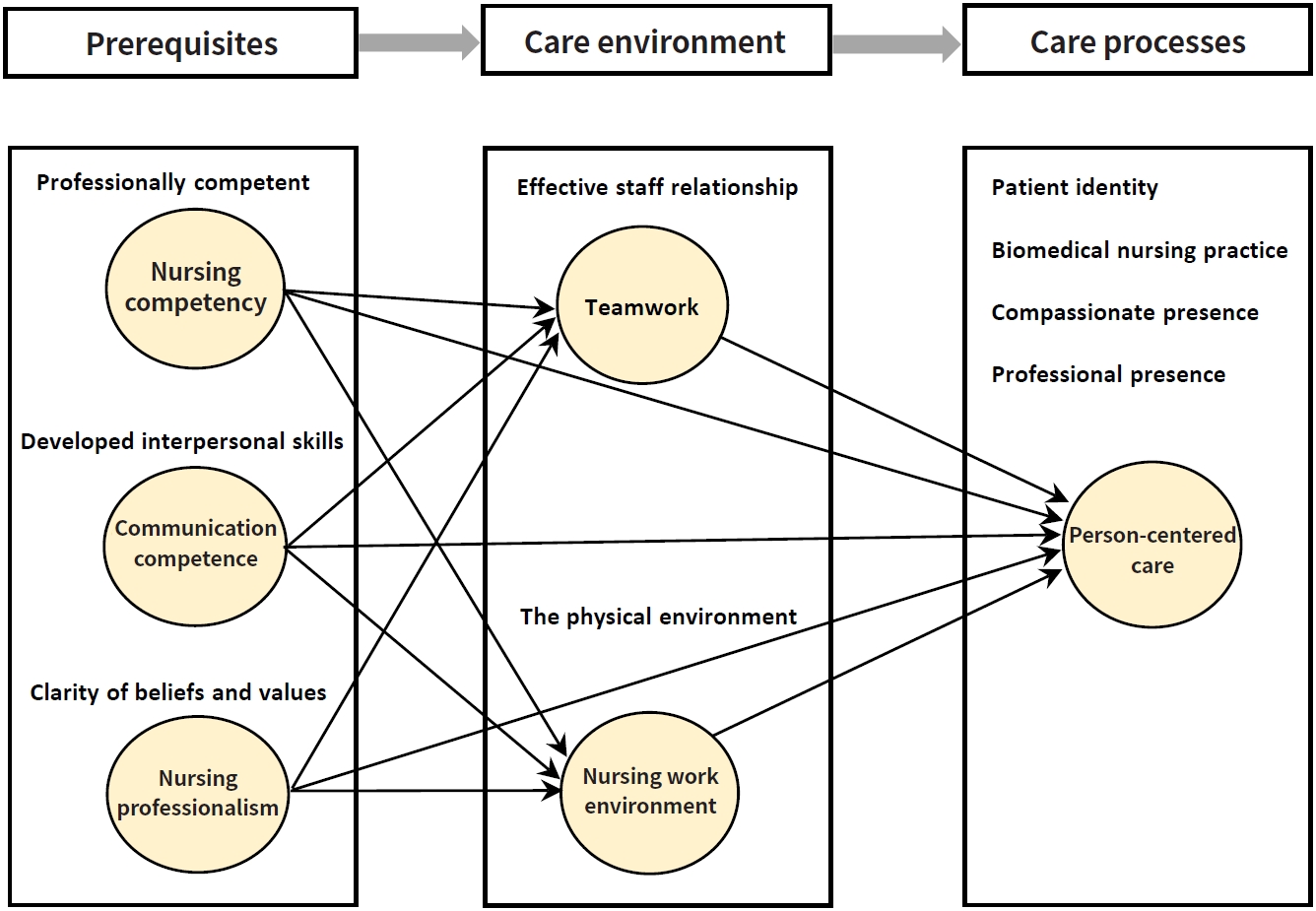
An integrated causal model was developed based on McCormack and McCance’s [
8] Person-Centered Nursing Theory and the four attributes of person-centered critical care nursing proposed by Jakimowicz and Perry [
12]. McCormack and McCance [
8] argue that person-centered outcomes arise from care processes shaped by nurses’ prerequisites and the care environment. In this study, prerequisites include nursing competency, communication competence, and nursing professionalism, while the care environment encompasses teamwork and the nursing work environment. Jakimowicz and Perry [
12] conceptualized ICU PCC as the application of advanced knowledge and technical expertise to preserve patient dignity and identity. Their four key attributes—patient identity, biomedical nursing practice, compassionate presence, and professional presence—are considered here as the care processes through which PCC is achieved. By integrating these frameworks, this study proposes a hypothetical model linking nurse characteristics, environmental factors, and PCC processes in ICUs (
Figure 1). The model’s pathways were subsequently tested for statistical significance and overall fit. This study thus aims to empirically validate an integrated causal model of PCC in ICUs, establishing a theoretical and empirical foundation for improving the quality of critical care nursing.
METHODS
1. Study Design
This cross-sectional study constructed a theoretical model of PCC for ICUs through a literature review and tested the model’s suitability by hypothesizing pathways using survey-based SEM. The study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
2. Setting and Samples
The sample consisted of 230 ICU nurses employed in the ICUs of a tertiary general hospital in South Korea, each with at least one year of direct patient care experience. According to Benner [
24], nurses’ skill levels are classified as novice, advanced beginner, competent, proficient, and expert. Nurses with at least one year of clinical experience are generally categorized as advanced beginners or are transitioning into the competent stage, during which they can provide nursing care with greater stability and autonomy in clinical settings. In addition, previous studies have demonstrated that clinical experience in ICUs positively influences the practice of PCC [
15,
20]. Based on these findings, a minimum of one year of ICU experience was established as an inclusion criterion.
Although there is no universal standard for determining sample size in SEM, the minimum number of participants recommended for the maximum likelihood estimation method, which is the most commonly used approach in structural modeling, is between 100 and 150. In general, a sample size of 200 is considered adequate for most structural models [
25]. Therefore, this study included 230 participants to account for potential dropout.
1) Person-centered care
The Person-Centered Critical Care Nursing scale, originally developed for ICU nurses by Kang et al. [
7], was used to measure the PCC process. The instrument consists of 15 items across four domains: compassion (4 items), individuality (4 items), respect (4 items), and comfort (3 items). Each item is rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree), with higher scores indicating greater levels of PCC practice. Cronbach’s α for this study was .83.
2) Nursing competency
Nursing competency was assessed using an instrument adapted by Kim [
26], based on Jang’s [
27] four-stage clinical career development model encompassing 13 nursing competencies. The tool includes 13 items across four domains: scientific nursing competency (3 items), ethical nursing competency (2 items), personal nursing competency (3 items), and esthetical nursing competency (5 items). Each item is rated on a 4-point Likert scale (1=disagree to 4=strongly agree), with higher scores reflecting higher nursing competency. Cronbach’s α for this study was .90.
3) Communication competence
Communication competence was measured using the Global Interpersonal Communication Competence Scale developed by Hur [
28]. The scale comprises 15 items rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree), with higher scores indicating greater communication competence. Cronbach’s α in this study was .85.
4) Nursing professionalism
Nursing professionalism was measured using the Nursing Professional Values Scale developed by Yeun et al. [
29]. The instrument includes 29 items across five domains: originality of nursing (3 items), roles of nursing service (4 items), professionalism of nursing (5 items), social awareness (8 items), and self-concept of the profession (9 items). The nursing originality domain contains reverse-scored items. Each item is rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree), with higher scores indicating more firmly established professional nursing intuition. Cronbach’s α in this study was .94.
5) Teamwork
Teamwork was assessed using the Teamwork Perceptions Questionnaire developed by the Agency for Healthcare Research and Quality and the U.S. Department of Defense [
30], using the Korean version translated and validated by Hwang and Ahn [
31]. This tool includes 35 items across five domains: team structure (7 items), leadership (7 items), situation monitoring (7 items), mutual support (7 items), and communication (7 items). Each item is rated on a 5-point Likert scale (1=strongly disagree to 5=strongly agree), with higher scores representing more positive perceptions of teamwork. The Cronbach’s α value obtained in this study was .96.
6) Nursing work environment
The Practice Environment Scale of the Nursing Work Index developed by Lake [
32] and translated and validated in Korean by Cho et al. [
33] was used to assess the nursing work environment. The scale consists of 29 items across five domains: nurse participation in hospital affairs (9 items), nursing foundations for quality of care (9 items), nurse manager ability, leadership, and support for nurses (4 items), staffing and resource adequacy (4 items), and collegial nurse-physician relationships (3 items). Each item is rated on a 4-point Likert scale (1=strongly disagree to 4=strongly agree), with higher scores reflecting more positive perceptions of the nursing work environment. Cronbach’s α in this study was .96.
Data were collected from March 2 to March 30, 2023. An actively operating online nursing community with over 500,000 members was selected. The purpose and procedures of the study were explained to the community administrator, and permission was obtained. A recruitment notice was then posted to invite participants, and the online survey was distributed to those who voluntarily expressed their intent to participate. Participants provided informed consent via the online link before completing the survey.
5. Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of Chung-Ang University (IRB No.: 1041078-20221231-HR-033). The study was conducted online, and participants were allowed to proceed with the survey only after reading an explanatory statement containing information on the study purpose, content, procedures, confidentiality, voluntary participation, withdrawal rights, and consent.
6. Data Analysis
Data were analyzed using SEM with IBM SPSS ver. 26.0 and AMOS ver. 25.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize participants’ characteristics and study variables, and instrument reliability was evaluated using Cronbach’s α. Univariate normality was assessed through means, standard deviations, skewness, and kurtosis in IBM SPSS, while multivariate normality was examined in AMOS. Convergent and discriminant validity were tested using confirmatory factor analysis. Model fit was assessed using the root mean square residual (RMR), standardized root mean square residual (SRMR), goodness-of-fit index (GFI), adjusted goodness-of-fit index (AGFI), Tucker–Lewis index (TLI), comparative fit index (CFI), and root mean square error of approximation (RMSEA). The significance of direct, indirect, and total effects was examined through bootstrapping procedures.
RESULTS
1. Participant Characteristics and Degree of Person-Centered Care Based on General Characteristics
The general characteristics of the participants and the degree of PCC according to these characteristics are presented in
Table 1. The total number of participants was 230, including 203 women (88.3%) and 27 men (11.7%). The mean age was 29.84 years, with 126 participants (54.8%) aged 20–29 years and 92 participants (40.0%) aged 30–39 years.
PCC significantly differed by age (F=28.91, p=.014), highest level of education (F=12.21, p=.001), position (t=2.72, p=.011), shift type (t=3.56, p=.002), total clinical work experience (F=7.56, p<.001), and average monthly income (F=2.98, p=.020). Participants aged 40 years or older demonstrated higher PCC levels than those in their 20s or 30s. Those with a master’s degree reported higher PCC levels than participants with an associate or bachelor’s degree. Additionally, participants with more than 10 years of clinical experience exhibited higher PCC levels than those with 1–4 years of experience.
2. Confirmatory Factor Analysis of Measured Variables
A latent variable was considered to demonstrate convergent validity when its construct reliability exceeded 0.7 and the average variance extracted (AVE) was greater than 0.5 [
25]. In this study, the reliability coefficients of all subdomains met the threshold of 0.7, confirming adequate internal consistency. For the sub-variables of PCC—compassion, individuality, respect, and comfort—the AVE was 0.439, while the construct reliability was 0.751, thus satisfying the standard criterion for composite reliability and supporting convergent validity. An examination of the confidence intervals of the correlation coefficients revealed that none included 1.0, thereby confirming discriminant validity and demonstrating that each construct represented a distinct concept. As Malhotra [
34] noted, convergent validity may still be acceptable when AVE is below 0.5 if the composite reliability is 0.7 or higher, further supporting the adequacy of this measurement model.
The criteria for determining an acceptable model fit were as follows: χ²/df≤3, RMR≤.05, SRMR≤.08, GFI≥.90, AGFI≥.80, CFI and TLI≥.90, and RMSEA≤.05, with values below .08 also considered acceptable [
25]. The theoretical model in this study demonstrated an adequate level of fit: χ²/df=2.25, RMR=.02, SRMR=.06, GFI=.85, AGFI=.81, TLI=.91, CFI=.92, and RMSEA=.07. Overall, the model fit indices met or closely approximated the recommended criteria, indicating a satisfactory goodness of fit.
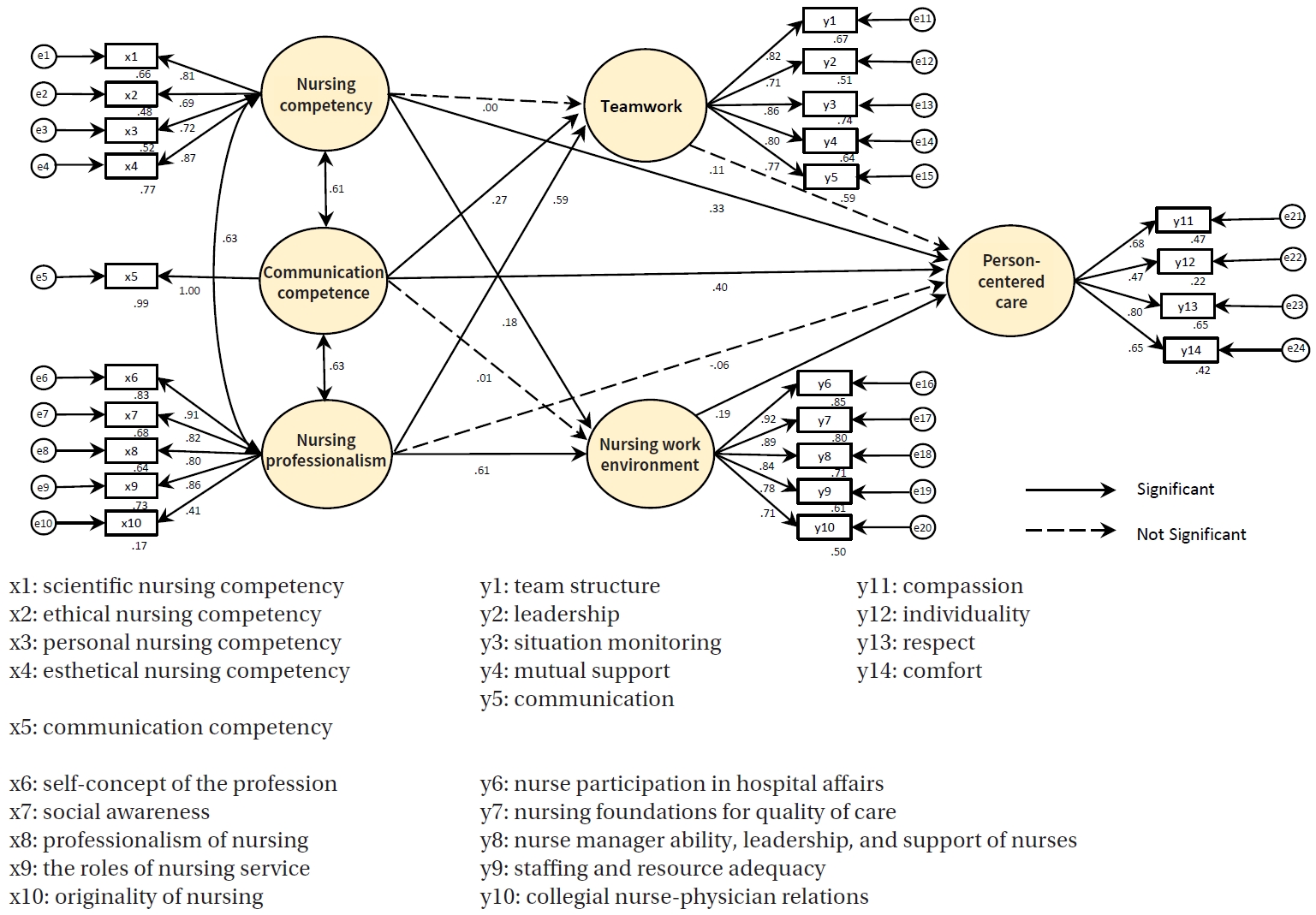
The final model was derived through a three-step process. In theoretical model 2, the relationship between nursing competency and teamwork, which was present in hypothetical model 1, was found to be non-significant and was therefore removed. In theoretical model 3, the relationship between communication competence and the nursing work environment was also excluded due to a lack of statistical significance. After excluding these non-significant paths, the model’s goodness of fit (χ²/df) changed minimally from 2.25 to 2.24, with no change in the other fit indices. Across all three theoretical models, seven paths remained statistically significant, and excluding the non-significant paths did not meaningfully alter the overall model fit. Therefore, theoretical model 1 was retained as the final model to fully consider the effects of each factor (
Table 2). Of the 11 hypothesized paths, seven were statistically significant (
Figure 2).
The direct, indirect, and total effects of the final model are shown in
Table 3. The PCC process was directly influenced by nursing competency, communication competence, and the nursing work environment. Nursing professionalism indirectly affected PCC through its influence on teamwork and the nursing work environment. Teamwork itself did not have a direct effect on PCC. The model’s explanatory power, with PCC as the endogenous variable, was 65.1% (SMC=.651).
DISCUSSION
This study developed a hypothetical model based on McCormack and McCance’s [
8] person-centered nursing theory and the attributes identified by Jakimowicz and Perry [
12] to examine factors influencing PCC in ICUs. Model testing was conducted in three steps, resulting in a final model in which seven of the 11 hypothesized paths were statistically significant. These findings provide a foundation for discussing the interrelationships among factors influencing PCC in ICUs.
This study found statistically significant pathways from nursing competency to both the nursing work environment and PCC, confirming that nursing competency plays a pivotal role in facilitating the delivery of PCC. Previous research similarly indicates that PCC is directly influenced by nursing competency [
23]. For example, nursing competency has been shown to have a significant positive correlation with the delivery of PCC and has been identified as a key influencing factor [
35]. These findings affirm that nursing competency is not merely an individual trait but a core foundation through which nurses translate clinical expertise into patient-centered interactions and outcomes. Interestingly, nursing competency did not have a direct effect on teamwork. Effective teamwork arises from interdependent collaboration, open communication, and shared decision-making, which contribute to positive outcomes for patients, organizations, and staff alike [
36]. Therefore, enhancing individual competence alone does not automatically lead to improved teamwork. To foster effective teamwork, efforts to strengthen nurses’ competencies must be accompanied by organizational support, including the establishment of collaborative systems and a culture that promotes mutual respect and cooperation.
Communication competence also emerged as a key determinant of PCC, underscoring the crucial role of interpersonal skills in high-acuity care settings. Previous studies have reported a significant positive correlation between communication competence and PCC [
6]. Whether viewed through an ecological lens [
15] or in adult ICU contexts [
2], communication consistently mediates the quality and depth of nurse-patient relationships. These findings reaffirm the importance of communication competence in intensive care nursing. To enhance the quality of nursing care in ICUs, specific strategies are required to strengthen nurses’ communication competencies.
Although nursing professionalism did not directly affect PCC in the model, it showed a significant indirect effect through the nursing work environment. This finding suggests that nursing professionalism enhances PCC by fostering a supportive and ethically grounded organizational culture. Nursing professionalism exhibited statistically significant pathways to both teamwork and the work environment, aligning with previous research showing that professional values influence organizational dynamics and job performance. Establishing nursing professionalism positively contributes to the delivery of high-quality nursing care and the effective performance of nursing duties [
29].
The study also found that teamwork did not have a direct effect on PCC, which contrasts with earlier findings that reported a significant positive relationship between teamwork and PCC [
15,
21,
37]. One possible explanation is that the participants’ teamwork levels were already uniformly high, reducing variability and diminishing its predictive power for PCC outcomes. As Rosen et al. [
38] emphasized, the effects of teamwork cannot be explained solely by team competencies but are also shaped by complex organizational structures and cultures. Similarly, the current findings suggest that institutional culture and organizational characteristics may mediate the relationship between teamwork and PCC. The results therefore highlight the structural dimensions of organizational culture and work systems. Effective implementation of teamwork requires a multidimensional approach encompassing both cultural and structural supports. Future studies should thus explore organizational culture and structural variables to provide a more comprehensive understanding of how teamwork influences PCC.
Furthermore, this study found that the nursing work environment had a statistically significant direct effect on PCC, indicating that the pathway from the nursing work environment to the delivery of PCC is meaningful. This finding aligns with prior research involving nurses in COVID-19–dedicated hospitals, which also demonstrated a significant influence of the nursing work environment on PCC [
20]. These results highlight the crucial role of organizational culture and environmental factors in shaping nurses’ PCC and underscore that fostering a high-quality nursing work environment is essential for promoting PCC [
39].
Overall, this study confirmed that communication competence, nursing competency, and the nursing work environment are influential determinants of ICU nurses’ PCC delivery. The implications for practice are threefold. First, structured communication training programs are necessary to enhance ICU nurses’ communication competence [
2,
15]. In Denmark, a communication education program for healthcare professionals significantly improved self-efficacy, demonstrating the effectiveness of structured training in enhancing communication competence [
40]. Simulation-based training and interprofessional communication programs should therefore be implemented. Second, continuous professional development and the establishment of practical support systems are vital to strengthening nursing competency. Because ICU nursing requires advanced clinical judgment and specialized expertise, professional education in this setting is of paramount importance. Studies have shown that adequate training for ICU nurses improves both patient outcomes and operational efficiency [
41]. Practical competency should be systematically reinforced through advanced training, case-based learning, simulation education, and mentoring. Third, organizational investment in improving the nursing work environment is essential. High workload intensity and emotional strain directly affect the quality of nursing care. Therefore, building a stable and sustainable work environment requires adequate staffing, emotional support, and reinforcement of teamwork and leadership [
39].
This study holds practical value and clinical applicability as it presents concrete strategies and actionable measures relevant to intensive care nursing practice. By identifying key factors that enhance the delivery of PCC, these findings provide foundational data for future ICU nursing education and program development. Because there is currently no validated instrument to directly assess PCC among hospitalized ICU patients, the theoretical framework of McCormack and McCance’s [
8] person-centered nursing theory and the four attributes of critical care nursing proposed by Jakimowicz and Perry [
12] were adopted. Accordingly, ICU nurses’ delivery of PCC was used as an evaluative indicator. Nevertheless, the study’s reliance on voluntary online recruitment may have introduced limitations, such as potential selection bias and reduced representativeness of the broader ICU nursing population.
CONCLUSION
This study analyzed the causal relationships among factors influencing PCC using SEM and proposed an integrated model explaining the mechanisms underlying PCC. The results identified nurses’ communication competence, nursing competency, and nursing work environment as the most influential factors significantly affecting the delivery of PCC. Accordingly, three practical measures are recommended to enhance the implementation of PCC: (1) the development of practice-oriented educational programs designed to strengthen ICU nurses’ communication competence; (2) the continuous and systematic integration of educational curricula with practice-based learning to advance nurses’ competencies and professional development; and (3) the implementation of organizational support measures to improve the nursing work environment, including optimal staffing levels, physical environment enhancement, and the cultivation of a positive workplace culture. Future research should aim to develop reliable measurement tools for systematically evaluating the effectiveness of PCC in critically ill patients. Additionally, educational and experimental intervention studies are needed to assess the efficacy of the proposed strategies for improving PCC.
-
CONFLICTS OF INTEREST
Kisook Kim, a contributing editor of the Korean Journal of Adult Nursing, was not involved in the editorial evaluation or decision to publish this article. The remaining author has declared no conflicts of interest.
-
AUTHORSHIP
Study conception and design acquisition - KK and SK; data collection - KK and SK; analysis and interpretation of the data - KK and SK; drafting and critical revision of the manuscript - KK and SK.
-
FUNDING
None.
-
ACKNOWLEDGEMENT
This article is a revision of the Sunmi Kwon’s doctoral thesis dissertation from Chung-Ang University.
-
DATA AVAILABILITY STATEMENT
Data sharing is not applicable to this article.
Figure 1.Theoretical framework of person-centered care in intensive care unit settings.
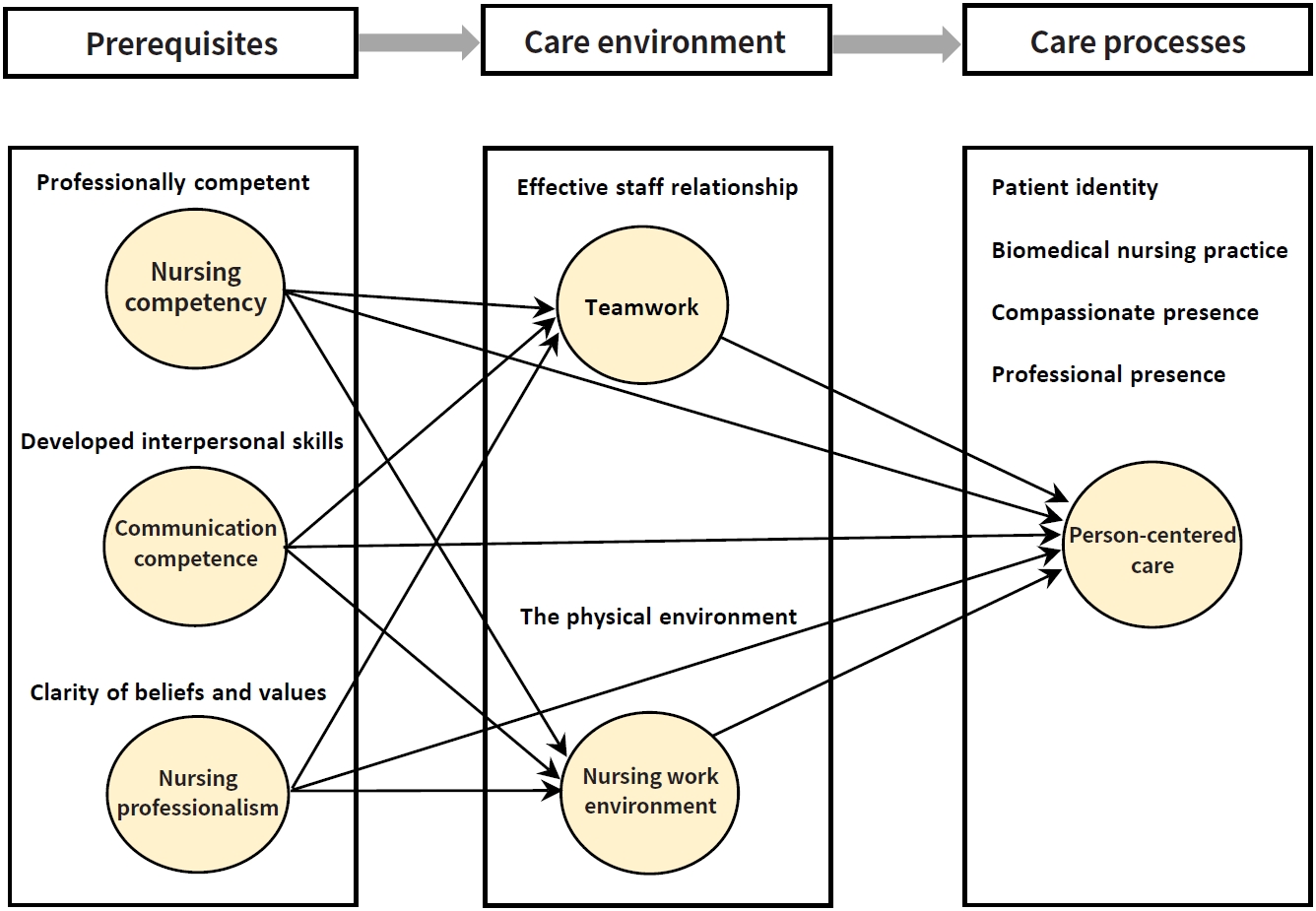
Figure 2.Path diagram of the final model.
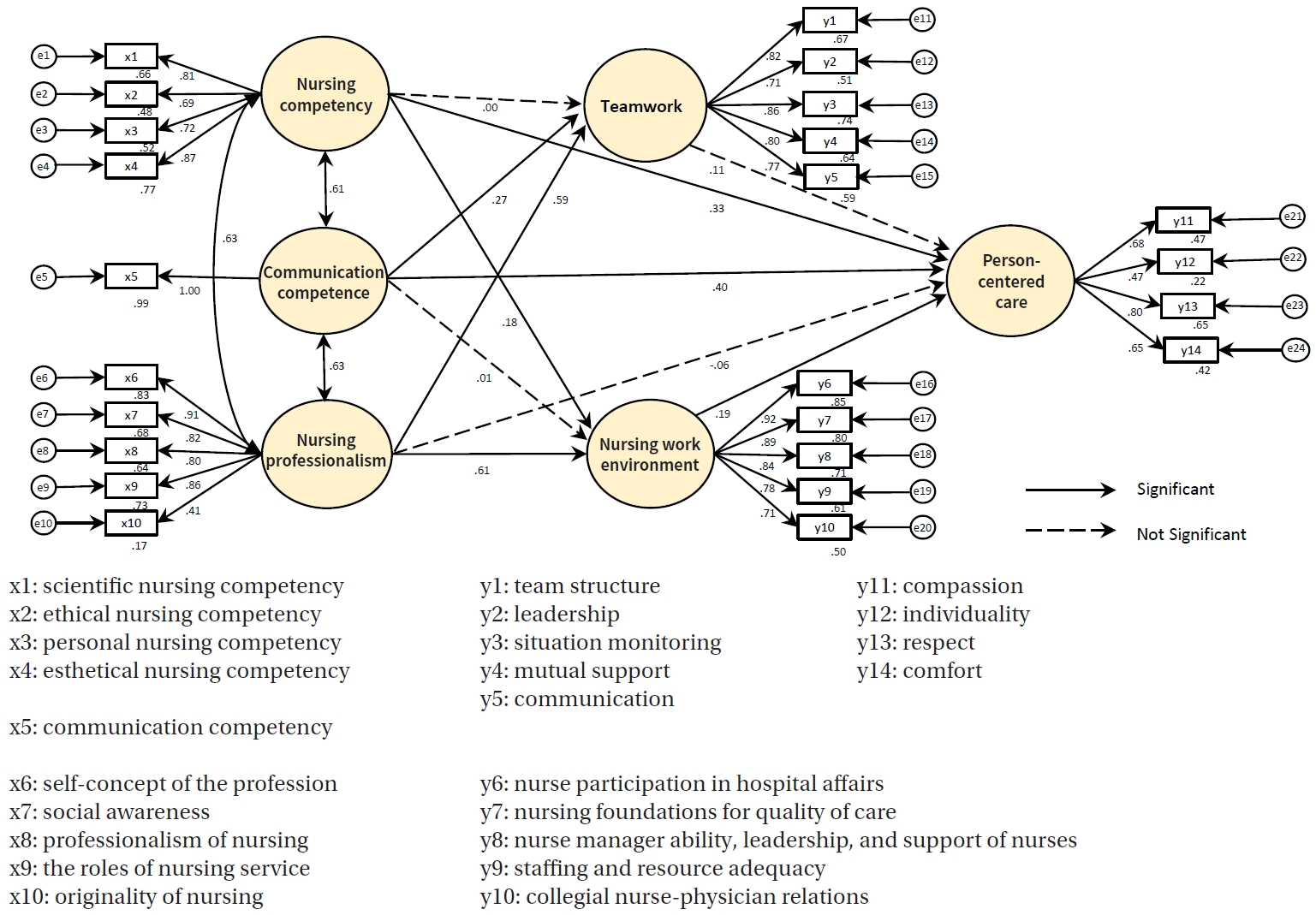
Table 1.Participant Characteristics and Degree of Person-Centered Care Based on General Characteristics (N=230)
|
Variables |
Categories |
n (%) |
M±SD |
t/F (p) Scheffé |
|
Gender |
Men |
27 (11.74) |
3.64±0.37 |
0.59 (.557) |
|
Women |
203 (88.26) |
3.58±0.48 |
|
Age (year) |
20–29a
|
126 (54.78) |
3.53±0.41 |
28.91 (.014)
c>a, c>b |
|
30–39b
|
92 (40.00) |
3.60±0.49 |
|
≥40c
|
12 (5.22) |
4.11±0.63 |
|
Marital status |
Unmarried |
184 (80.00) |
3.59±0.48 |
0.02 (.981) |
|
Married |
46 (20.00) |
3.59±0.42 |
|
Children |
0 |
205 (89.13) |
3.59±0.47 |
0.23 (.792) |
|
1 |
8 (3.48) |
3.57±0.49 |
|
≥2 |
17 (7.39) |
3.51±0.44 |
|
Religion |
Christian |
27 (11.74) |
3.62±0.44 |
0.89 (.448) |
|
Catholic |
16 (6.96) |
3.74±0.39 |
|
Buddhist |
18 (7.83) |
3.49±0.43 |
|
None |
169 (73.47) |
3.58±0.49 |
|
Educational background |
Collegea
|
7 (3.04) |
3.28±0.34 |
12.21 (.001)
c>a, c>b |
|
Universityb
|
190 (82.61) |
3.53±0.41 |
|
≥Master’s degreec
|
33 (14.35) |
3.99±0.58 |
|
Position |
Staff nurse |
205 (89.13) |
3.54±0.41 |
2.72 (.011) |
|
Charge nurse |
25 (10.87) |
3.95±0.73 |
|
Shift type |
3 shifts |
212 (92.17) |
3.54±0.42 |
3.56 (.002) |
|
2 shifts |
18 (7.83) |
4.13±0.70 |
|
Average number of patients per shift (person) |
≤2 |
136 (59.13) |
3.63±0.50 |
1.54 (.216) |
|
3 |
67 (29.13) |
3.55±0.40 |
|
≥4 |
27 (11.74) |
3.47±0.45 |
|
Total clinical experience (year) |
1–4a
|
115 (50.00) |
3.52±0.39 |
7.56 (<.001)
c>a, c>b |
|
5–9b
|
75 (32.61) |
3.56±0.45 |
|
≥10c
|
40 (17.39) |
3.84±0.63 |
|
Current department work experience (year) |
1–4 |
159 (69.13) |
3.54±0.40 |
2.94 (.068) |
|
5–9 |
58 (25.22) |
3.74±0.62 |
|
≥10 |
13 (5.65) |
3.48±0.41 |
|
Average monthly income (10,000 KRW) |
200–299 |
13 (5.65) |
3.47±0.34 |
2.98 (.020) |
|
300–349 |
106 (46.09) |
3.53±0.44 |
|
350–399 |
76 (33.04) |
3.72±0.47 |
|
400–449 |
22 (9.57) |
3.61±0.50 |
|
≥450 |
13 (5.65) |
3.36±0.59 |
|
Department (intensive care unit) |
Medial |
129 (56.09) |
3.60±0.51 |
0.35 (.844) |
|
Surgical |
59 (25.65) |
3.56±0.36 |
|
Neonatal |
21 (9.13) |
3.54±0.32 |
|
Pediatric |
10 (4.35) |
3.71±0.62 |
|
Integrated |
11 (4.78) |
3.52±0.64 |
Table 2.
|
Exogenous variables |
|
Endogenous variables |
Unstandardized coefficient |
Standardized coefficient |
SE |
CR |
p
|
|
Nursing competency |
→ |
Teamwork |
0.00 |
0.00 |
0.07 |
–0.00 |
.999 |
|
→ |
Nursing work environment |
0.24 |
0.18 |
0.10 |
2.29 |
.022 |
|
→ |
PCC |
0.32 |
0.33 |
0.09 |
3.69 |
<.001 |
|
Communication competence |
→ |
Teamwork |
0.27 |
0.27 |
0.07 |
3.91 |
<.001 |
|
→ |
Nursing work environment |
0.01 |
0.01 |
0.10 |
0.11 |
.916 |
|
→ |
PCC |
0.41 |
0.40 |
0.09 |
4.78 |
<.001 |
|
Nursing professionalism |
→ |
Teamwork |
0.44 |
0.59 |
0.06 |
7.36 |
<.001 |
|
→ |
Nursing work environment |
0.65 |
0.61 |
0.08 |
7.72 |
<.001 |
|
→ |
PCC |
–0.05 |
–0.06 |
0.09 |
–0.53 |
.597 |
|
Teamwork |
→ |
PCC |
0.11 |
0.11 |
0.10 |
1.05 |
.292 |
|
Nursing work environment |
→ |
PCC |
0.14 |
0.19 |
0.06 |
2.16 |
.031 |
Table 3.Standardized Direct, Indirect, and Total Effects of the Model (N=230)
|
Endogenous variables |
Exogenous variables |
Effect size (p) |
SMC |
|
Direct effect |
Indirect effect |
Total effect |
|
PCC |
Nursing competency |
0.33 (<.001) |
0.03 (.254) |
0.36 (<.001) |
.651 |
|
Nursing professionalism |
–0.06 (.650) |
0.18 (.034) |
0.11 (.255) |
|
Communication competence |
0.40 (<.001) |
0.03 (.434) |
0.43 (<.001) |
|
Teamwork |
0.11 (.408) |
|
0.11 (.408) |
|
Nursing work environment |
0.19 (.046) |
0.19 (.046) |
|
Teamwork |
Nursing competency |
0.00 (.991) |
|
0.00 (.991) |
.617 |
|
Nursing professionalism |
0.59 (<.001) |
0.59 (<.001) |
|
Communication competence |
0.27 (.001) |
0.27 (.001) |
|
Nursing work environment |
Nursing competency |
0.18 (.051) |
|
0.18 (.051) |
.548 |
|
Nursing professionalism |
0.61 (<.001) |
0.61 (<.001) |
|
Communication competence |
0.01 (.915) |
0.01 (.915) |
REFERENCES
- 1. Marshall JC, Bosco L, Adhikari NK, Connolly B, Diaz JV, Dorman T, et al. What is an intensive care unit? A report of the task force of the World Federation of Societies of Intensive and Critical Care Medicine. J Crit Care. 2017;37:270-6. https://doi.org/10.1016/j.jcrc.2016.07.015
- 2. Joo YS, Jang YS. Predictors of person-centered care among nurses in adult intensive care units. J Korean Clin Nurs Res. 2022;28(1):34-44. https://doi.org/10.22650/JKCNR.2022.28.1.34
- 3. Jakimowicz S, Perry L, Lewis J. An integrative review of supports, facilitators and barriers to patient-centred nursing in the intensive care unit. J Clin Nurs. 2017;26(23-24):4153-71. https://doi.org/10.1111/jocn.13957
- 4. Ahmadi N, Sasangohar F, Yang J, Yu D, Danesh V, Klahn S, et al. Quantifying workload and stress in intensive care unit nurses: preliminary evaluation using continuous eye-tracking. Hum Factors Health. 2024;66(3):714-28. https://doi.org/10.1177/00187208221085335
- 5. Banda Z, Simbota M, Mula C. Nurses' perceptions on the effects of high nursing workload on patient care in an intensive care unit of a referral hospital in Malawi: a qualitative study. BMC Nurs. 2022;21(1):136. https://doi.org/10.1186/s12912-022-00918-x
- 6. Kang HS, Seo M. The factors affecting person-centered care nursing in intensive care unit nurses. J Korean Crit Care Nurs. 2021;14(3):14-25. https://doi.org/10.34250/jkccn.2021.14.3.14
- 7. Kang J, Cho YS, Jeong YJ, Kim SG, Yun S, Shim M. Development and validation of a measurement to assess person-centered critical care nursing. J Korean Acad Nurs. 2018;48(3):323-34. https://doi.org/10.4040/jkan.2018.48.3.323
- 8. McCormack B, McCance T. Person-centred nursing: theory and practice. Oxford: Wiley-Blackwell; 2010.
- 9. Lusk JM, Fater K. A concept analysis of patient-centered care. Nurs Forum. 2013;48(2):89-98. https://doi.org/10.1111/nuf.12019
- 10. Hakansson Eklund J, Holmstrom IK, Kumlin T, Kaminsky E, Skoglund K, Hoglander J, et al. "Same same or different?" A review of reviews of person-centered and patient-centered care. Patient Educ Couns. 2019;102(1):3-11. https://doi.org/10.1016/j.pec.2018.08.029
- 11. Morgan S, Yoder LH. A concept analysis of person-centered care. J Holist Nurs. 2012;30(1):6-15. https://doi.org/10.1177/0898010111412189
- 12. Jakimowicz S, Perry L. A concept analysis of patient-centred nursing in the intensive care unit. J Adv Nurs. 2015;71(7):1499-517. https://doi.org/10.1111/jan.12644
- 13. Pirhonen L, Gyllensten H, Olofsson EH, Fors A, Ali L, Ekman I, et al. The cost-effectiveness of person-centred care provided to patients with chronic heart failure and/or chronic obstructive pulmonary disease. Health Policy Open. 2020;1:100005. https://doi.org/10.1016/j.hpopen.2020.100005
- 14. Hong HJ, Kang J. A qualitative content analysis of the person-centered care experienced by critical care patients. J Korean Crit Care Nurs. 2018;11(2):21-33.
- 15. Lee Y, Kim Y. Influencing factors on performance of person-centered care among intensive care unit nurses: an ecological perspective. Korean J Adult Nurs. 2021;33(5):522-31. https://doi.org/10.7475/kjan.2021.33.5.522
- 16. Youn H, Lee M, Jang SJ. Person-centred care among intensive care unit nurses: a cross-sectional study. Intensive Crit Care Nurs. 2022;73:103293. https://doi.org/10.1016/j.iccn.2022.103293
- 17. McCormack B, McCance TV. Development of a framework for person-centred nursing. J Adv Nurs. 2006;56(5):472-9. https://doi.org/10.1111/j.1365-2648.2006.04042.x
- 18. McCance T, McCormack B, Dewing J. An exploration of person-centredness in practice. Online J Issues Nurs. 2011;16(2):1. https://doi.org/10.3912/OJIN.Vol16No02Man01
- 19. Edvardsson D, Fetherstonhaugh D, Nay R, Gibson S. Development and initial testing of the Person-centered Care Assessment Tool (P-CAT). Int Psychogeriatr. 2010;22(1):101-8. https://doi.org/10.1017/s1041610209990688
- 20. Jung TM, Kim KA. The influence of nursing professionalism, communication competence and nursing work environment of dedicated COVID-19 hospital nurse on person-centered care. J Home Care Nurs. 2022;29(2):165-74. https://doi.org/10.22705/jkashcn.2022.29.2.165
- 21. Kim K, Kwon S. Factors influencing person-centered care among nurses in COVID-19 special care units at tertiary general hospitals: a cross-sectional descriptive study. Korean J Adult Nurs. 2023;35(2):127-37. https://doi.org/10.7475/kjan.2023.35.2.127
- 22. Jeong H, Park M. A predictive model on patient-centered care of hospital nurses in Korea. J Korean Acad Nurs. 2019;49(2):191-202. https://doi.org/10.4040/jkan.2019.49.2.191
- 23. Bae YH, Yeom HA. Structural equation modeling of person-centered nursing in hospital nurses. Healthcare (Basel). 2022;10(3):514. https://doi.org/10.3390/healthcare10030514
- 24. Benner P. From novice to expert: excellence and power in clinical nursing practice. Menlo Park, CA: Addison-Wesley; 1984.
- 25. Woo JP. Understanding of structural equation modeling and its concepts. Seoul: Hannarae Publisher; 2022.
- 26. Kim SJ. A comparison of affecting variables on nursing competency between nursing home nurses and hospital nurses [master’s thesis]. Daegu: Daegu Catholic University; 2009.
- 27. Jang KS. A study on establishment of clinical career development model of nurses [dissertation]. Seoul: Yonsei University; 2000.
- 28. Hur GH. Construction and validation of a global interpersonal communication competence scale. Korean J Journalism Commun. 2003;47(6):380-408.
- 29. Yeun EJ, Kwon YM, Ahn OH. Development of a nursing professional values scale. J Korean Acad Nurs. 2005;35(6):1091-100. https://doi.org/10.4040/jkan.2005.35.6.1091
- 30. Battles J, King HB. TeamSTEPPS Teamwork Perceptions Questionnaire (T-TPQ) Manual [Internet]. Washington, DC: American Institutes for Research; 2010 [cited 2022 August 12]. Available from: http://teamstepps.ahrq.gov/Teamwork_Perception_Questionnaire.pdf
- 31. Hwang JI, Ahn J. Teamwork and clinical error reporting among nurses in Korean hospitals. Asian Nurs Res. 2015;9(1):14-20. https://doi.org/10.1016/j.anr.2014.09.002
- 32. Lake ET. Development of the practice environment scale of the Nursing Work Index. Res Nurs Health. 2002;25(3):176-88. https://doi.org/10.1002/nur.10032
- 33. Cho E, Choi M, Kim EY, Yoo IY, Lee NJ. Construct validity and reliability of the Korean version of the practice environment scale of nursing work index for Korean nurses. J Korean Acad Nurs. 2011;41(3):325-32. https://doi.org/10.4040/jkan.2011.41.3.325
- 34. Malhotra NK. Marketing research: an applied orientation. 6th ed. Upper Saddle River, NJ: Prentice Hall; 2010.
- 35. Ahn JY, Eun Y. The effect of nursing competence on patient-centered care among nurses caring for patients with chronic disease: the mediating effect of burnout and the moderating effect of nursing work environment. Korean J Adult Nurs. 2021;33(2):134-44. https://doi.org/10.7475/kjan.2021.33.2.134
- 36. Xyrichis A, Ream E. Teamwork: a concept analysis. J Adv Nurs. 2008;61(2):232-41. https://doi.org/10.1111/j.1365-2648.2007.04496.x
- 37. Lee HA, Hyun MS, Park JH, Seo EJ. Workload, teamwork, compassion competence, and person-centered critical care nursing among critical care nurses. J Korean Crit Care Nurs. 2025;18(2):14-25. https://doi.org/10.34250/jkccn.2025.18.2.14
- 38. Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, et al. Teamwork in healthcare: key discoveries enabling safer, high-quality care. Am Psychol. 2018;73(4):433-50. https://doi.org/10.1037/amp0000298
- 39. Nagel C, Westergren A, Persson SS, Lindstrom PN, Bringsen A, Nilsson K. Nurses’ work environment during the COVID-19 pandemic in a person-centred practice: a systematic review. Sustainability. 2022;14(10):5785. https://doi.org/10.3390/su14105785
- 40. Wolderslund M, Kofoed PE, Ammentorp J. The effectiveness of a person-centred communication skills training programme for the health care professionals of a large hospital in Denmark. Patient Educ Couns. 2021;104(6):1423-30. https://doi.org/10.1016/j.pec.2020.11.018
- 41. Perez-Talavera C. Nursing specialization in intensive care: a scoping review. Enferm Intensiva (Engl Ed). 2025;36(2):500529. https://doi.org/10.1016/j.enfie.2025.500529


 E-SUBMISSION
E-SUBMISSION
