The Effects of an Individual and Family Self-Management Program for Slowing Disease Progression via a Mobile Application on Self-Management Behaviors and Clinical Outcomes in Patients with Stage 3 Chronic Kidney Disease in Thailand: A Quasi-Experimental Study
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc-nd/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Stage 3 chronic kidney disease (CKD) is highly prevalent and often progresses to end-stage renal disease without effective self-management. This study examined the effects of an Individual and Family Self-Management Program delivered via a mobile communication application on self-management behaviors and clinical outcomes among patients with stage 3 CKD.
Methods
A 12-week quasi-experimental study with a pretest-posttest control group design was conducted among 50 patients with stage 3 CKD at a tertiary hospital in Thailand, between January and May 2024. The intervention group received a self-management program grounded in Individual and Family Self-Management Theory and delivered via the LINE chatbot. The program included educational content, self-regulation strategies, and structured family support, while the control group received usual care. Outcomes included self-management behaviors, estimated glomerular filtration rate (eGFR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and hemoglobin A1c (HbA1c). Analysis of covariance was used to adjust for baseline differences.
Results
After adjustment for baseline values, the intervention group showed significantly greater improvements in self-management behaviors (F=7.92, p < .05) and eGFR (F=52.92, p < .001) compared with the control group. Significant reductions were also observed in SBP (F=26.84, p < .001), DBP (F=12.61, p < .05), and HbA1c levels (F=7.74, p < .05).
Conclusion
A mobile-based Individual and Family Self-Management Program effectively improved self-management behaviors and key clinical outcomes among patients with stage 3 CKD, supporting the integration of family engagement and digital technology in chronic disease care.
Chronic kidney disease (CKD) is a major public health problem worldwide, including in Thailand, affecting more than 10% of the global population, or over 800 million individuals [1]. In Thailand, recent findings indicate that the prevalence of CKD among the Thai population has increased to 17.5%, corresponding to approximately 11.6 million individuals [2], and the number of deaths attributable to CKD is expected to continue rising. In 2020, a total of 10,758 deaths were attributed to CKD [3]. When CKD prevalence was examined by disease stage in the Thai population, stage 3 CKD was found to be the most common, accounting for as much as 43.38% of cases in 2024.
CKD cannot be completely cured once kidney deterioration has occurred, and without effective slowing of disease progression, CKD will advance to end-stage renal disease (ESRD), necessitating renal replacement therapy. CKD arises from multiple contributing factors. Evidence from the literature indicates that hypertension and elevated blood glucose levels are key predictive factors associated with declining glomerular filtration rate (GFR) and disease progression [4,5]. Patients with CKD and uncontrolled hypertension experience a GFR decline exceeding 4 mL/min/1.73 m² per year [6]. In addition, patients with CKD and poorly controlled blood glucose levels have a 2.51-fold higher risk of developing kidney failure compared with those whose blood glucose is well managed [7]. Consistent with these findings, data from the Nephrology Society of Thailand [8] indicate that most new patients receiving renal replacement therapy had diabetes (32.2%), followed by hypertension (29.2%).
The Nephrology Society of Thailand [8] and the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines [9] recommend comprehensive strategies to slow kidney deterioration in patients with stage 3 CKD. According to the KDIGO 2022 guideline, stage 3 CKD is defined as a moderate reduction in kidney function, characterized by an estimated glomerular filtration rate (eGFR) of 30–59 mL/min/1.73 m² sustained for at least three months. Recommended management strategies include blood pressure control, blood glucose control, health behavior modification, and adherence to prescribed medications. These self-management activities are essential for delaying disease progression. When patients engage effectively in these behaviors, renal function decline may be substantially slowed, thereby delaying progression to ESRD [9,10].
Although programs aimed at slowing kidney deterioration in patients with stage 3 CKD have been developed, many patients continue to engage in inappropriate behaviors that contribute to disease progression [11]. Previous studies have reported that 24% to 33% of patients with CKD are overweight or obese [12], while 11.1% do not engage in regular physical activity [13]. In addition, 89.6% continue to consume salty foods [14], 65.1% report excessive fat intake [13], and 80% demonstrate only moderate adherence to prescribed medication regimens [15]. Furthermore, 9.8% of patients smoke [16], and 10% engage in heavy alcohol consumption [17]. These findings underscore the persistent need for interventions that support patients with CKD in modifying risk behaviors to delay kidney deterioration.
A review of the literature on behavior modification programs designed to delay kidney deterioration indicates that effective interventions should integrate essential knowledge related to disease progression, tailor self-management strategies, enhance patients’ awareness of their capacity to adopt these behaviors, provide motivational counseling to facilitate behavior change, and incorporate social support [18]. However, many existing programs do not comprehensively address the guideline recommendations for slowing CKD progression established by KDIGO. In addition, although numerous programs target CKD across multiple disease stages, relatively few focus specifically on stage 3 CKD, despite its high prevalence. Furthermore, while most programs implemented in Thailand are conducted over a 12-week period and have demonstrated effectiveness, they often lack a critical component, social support, and do not fully encompass the recommended content outlined in the guidelines of the Nephrology Society of Thailand. Family members, in particular, play a vital role in supporting patients’ self-management behaviors. Collectively, these gaps present ongoing challenges for nurses in developing new programs that effectively delay kidney deterioration.
The current care model for patients with stage 3 CKD in Thailand primarily focuses on preventing progression to more advanced stages of the disease. Patients with stage 3 CKD typically receive care through scheduled follow-up appointments in outpatient departments. However, due to limited consultation time and constraints in healthcare service accessibility, patients often receive insufficient information to support effective self-management. Previous research has shown that individuals with stage 3 CKD receiving outpatient services obtain relatively limited guidance from healthcare providers [19]. In recent years, health innovations have been developed to improve patient access to healthcare services [20]. A national survey reported that 90.9% of the Thai population has internet access, and 99.4% use social networks for consultation and medical services, particularly through e-Health platforms [21].
Although previous intervention studies addressing CKD have been conducted, important gaps remain in adequately covering the guideline recommendations for slowing kidney deterioration established by the Nephrology Society of Thailand and KDIGO. In addition, family involvement in supporting behavioral changes aimed at slowing disease progression remains limited. The current care model for patients with CKD also restricts the amount of time available for healthcare services, further compounding these challenges. To address these gaps, this study developed an Individual and Family Self-Management Program based on Ryan and Sawin’s Individual and Family Self-Management Theory (IFSMT) [22]. The program was designed using a family-centered approach grounded in IFSMT. Social support from family members was deliberately incorporated because patients with stage 3 CKD often rely on family assistance for medication management, lifestyle modification, appointment adherence, and monitoring of clinical symptoms. Family members were encouraged to participate in educational activities, provide daily support, and reinforce self-management behaviors, thereby enhancing the feasibility and sustainability of behavior change.
The selection of dependent variables in this study was guided by their established relevance as behavioral and clinical indicators of CKD progression, in accordance with recommendations from KDIGO and national clinical practice guidelines. Self-management behaviors were included to capture a broad range of patient practices influencing disease control, including blood pressure regulation, glycemic management, lifestyle modification, and adherence to prescribed medications. eGFR was identified as the primary indicator of renal function and CKD staging, whereas systolic and DBP were incorporated because of their roles as major modifiable risk factors associated with accelerated renal deterioration. Hemoglobin A1c (HbA1c) was selected because glycemic control is a critical determinant of CKD progression among individuals with comorbid diabetes.
The self-management program evaluated in this study was designed to strengthen behaviors that mitigate kidney function decline through structured family participation, comprehensive alignment with the guidelines of the Nephrology Society of Thailand and KDIGO, and attention to individualized patient needs. Integration of a LINE-based chatbot was intended to enhance access to reliable health information and facilitate sustained engagement by both patients and family members. Collectively, these program components were designed to improve self-management capacity, slow disease progression, and reduce the overall burden of CKD. Accordingly, this study aimed to examine changes in self-management behaviors and clinical outcomes—including eGFR, systolic blood pressure (SBP), diastolic blood pressure (DBP), and HbA1c—within the intervention and control groups from baseline to follow-up, as well as to compare differences in these outcomes between groups following the intervention.
METHODS
1. Study Design
A 12-week quasi-experimental study was conducted to examine the effects of an Individual and Family Self-Management Program for slowing CKD progression, delivered via a mobile communication application, on self-management behaviors and clinical outcomes among patients with stage 3 CKD.
2. Setting and Samples
This study was conducted in the outpatient department of a tertiary hospital in Chonburi, Thailand. Participants were patients diagnosed by a physician with stage 3 CKD or those with an eGFR between 30 and 59 mL/min/1.73 m² for at least three months. Inclusion criteria were as follows: (1) age 18 years or older; (2) living with a family member who served as the primary caregiver; (3) presence of comorbid uncontrolled diabetes (HbA1c >7%) and/or uncontrolled hypertension (SBP ≥140 mmHg and/or DBP ≥90 mmHg); (4) intact orientation with no cognitive impairment; (5) ability to read and communicate in Thai; and (6) ownership of a smartphone capable of installing the LINE chatbot application. Participants were excluded if they changed their treatment regimen during the program, such as modifying blood glucose-lowering or antihypertensive medications, progressed from stage 3 CKD to a more advanced stage, or developed complications requiring urgent dialysis. Primary caregivers were eligible if they were aged 18 years or older, able to communicate in Thai, and had no hearing or visual impairments.
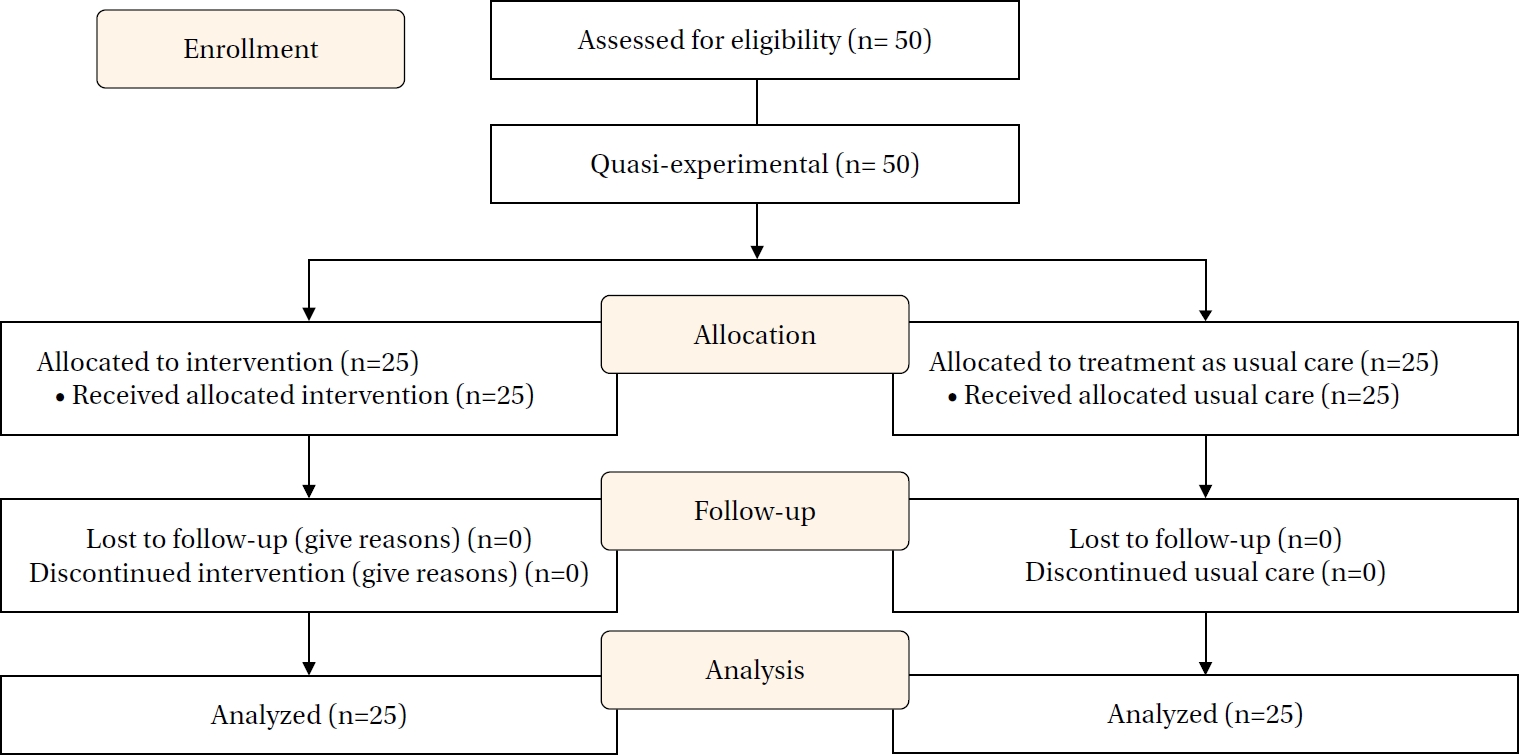
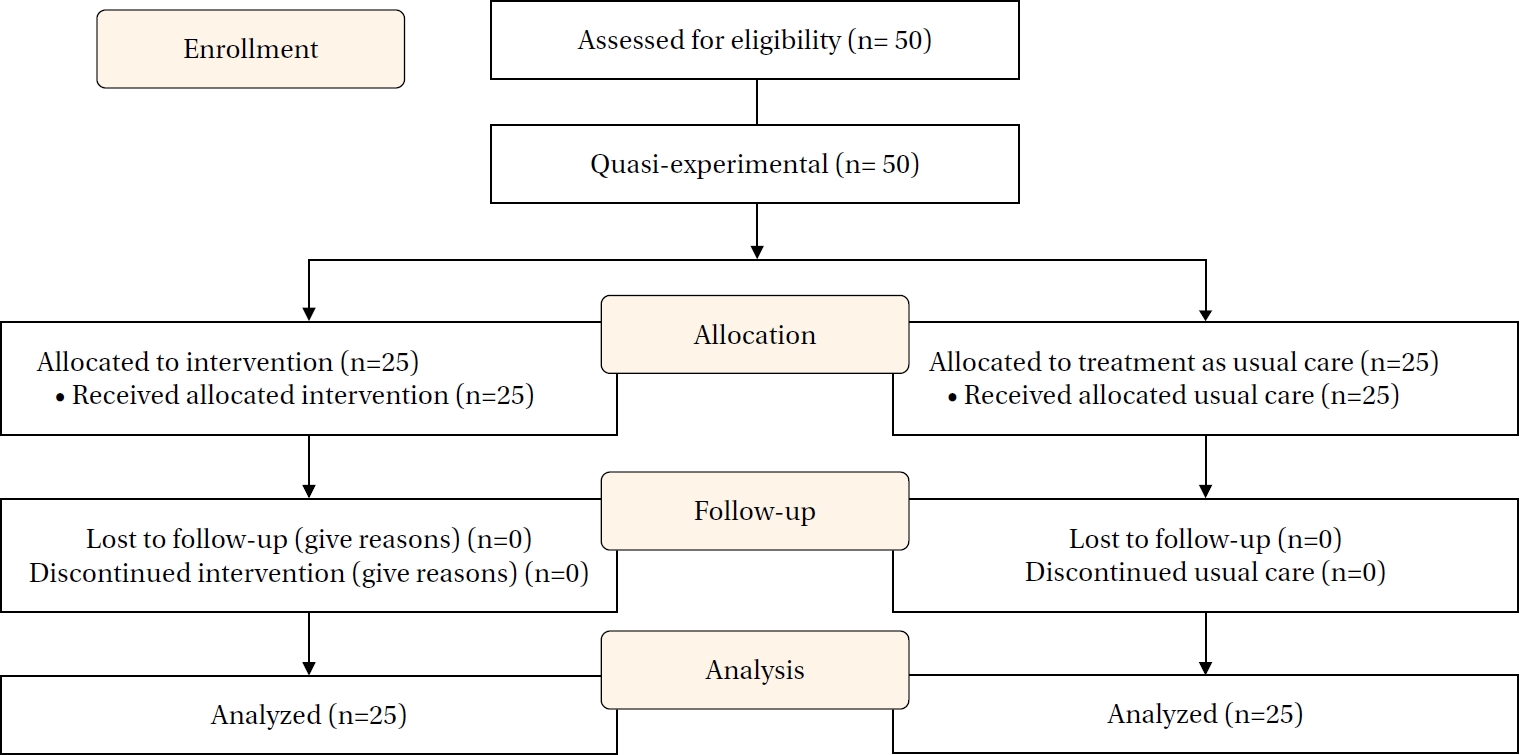
The sample size was calculated using the G*Power program ver. 3.1.9, based on the effect size reported in a previous study with a similar research design [23], which yielded an effect size of 3.29. Because this effect size was considered excessively large and resulted in an unrealistically small sample size, an alternative effect size of 0.80 was selected. This value represents a large effect size commonly accepted in health research [24]. The level of statistical significance (α) was set at .05, and statistical power was set at .80, using a one-tailed test. Based on these parameters, the required sample size was 21 participants per group, for a total of 42 participants. To compensate for potential attrition, the sample size was increased by 20% [25], resulting in 25 participants per group and a total sample of 50 participants. No participants withdrew during the study, yielding a final sample of 50 participants (Figure 1). All participants completed the 12-week study period, with no loss to follow-up in either group. Therefore, baseline comparisons between those retained and those lost to follow-up were not applicable.
3. Measurements/Instruments
1) Personal demographic and health status questionnaire
A personal demographic and health status questionnaire was used to collect baseline participant information. The demographic section consisted of six items assessing gender, age, education level, monthly income, income sufficiency, and primary caregiver status. Health status information was obtained using seven items, including weight, height, eGFR, HbA1c, and blood pressure measurements. Kidney function was assessed using eGFR calculated with the CKD-EPI equation based on standardized serum creatinine values. Glycemic control was evaluated using HbA1c levels. Laboratory data were retrieved from Burapha University Hospital and analyzed using standardized laboratory equipment certified by the Department of Medical Sciences, Ministry of Public Health. Blood pressure was measured using a digital blood pressure monitor that undergoes annual quality verification by a certified company in accordance with Ministry of Public Health medical device testing standards (TP-MMD-01). All blood pressure measurements were performed by the researcher in accordance with the guidelines of the Thai Hypertension Society [26]. Body mass index (BMI) was calculated from measured weight and height using the formula kg/m². Obesity classification followed the World Health Organization criteria for Asians, with BMI values of 25.00–29.99 kg/m² classified as obesity class I and BMI values ≥30.00 kg/m² classified as obesity class II. These classifications were used to describe baseline health characteristics in the study results.
2) Self-management behaviors for slowing CKD progression questionnaire
The self-management behaviors for slowing CKD progression questionnaire was developed by the research team based on guidelines from the Nephrology Society of Thailand [8], the Thai Hypertension Society [26], and the Diabetes Association of Thailand [27], as well as a comprehensive review of relevant literature on self-management strategies for patients with stage 3 CKD and uncontrolled diabetes and/or hypertension. The questionnaire was designed to assess behaviors related to slowing kidney deterioration and consisted of four domains: blood glucose control (4 items), blood pressure control (3 items), health behavior modification (22 items), and medication adherence (7 items), for a total of 36 items. Each item was rated on a 4-point Likert scale ranging from 1 (“never”) to 4 (“consistently”). Mean scores were calculated for each domain and for the overall scale. Higher mean scores indicated more consistent and effective engagement in CKD self-management behaviors, whereas lower scores reflected insufficient or inconsistent engagement. The theoretical mean score range for both domain-specific and total scores was 1.00 to 4.00. Content validity was evaluated by three experts, yielding a Content Validity Index of 0.86, which exceeds the acceptable standard of 0.80 [25]. Internal consistency reliability was assessed using Cronbach’s α coefficient, resulting in a value of .83, which is above the accepted threshold of .70 [28].
3) Research intervention instrument
The research intervention instrument was the Individual and Family Self-Management for Slowing CKD Progression Program, developed based on Ryan and Sawin’s IFSMT [22]. The program was designed to enhance participants’ capacity to manage stage 3 CKD through three core components: enhancement of knowledge and beliefs, development of self-regulation skills, and social facilitation.
4. Data Collection/Procedure
Data were collected between January and May 2024 at the outpatient department of Burapha University Hospital in Chonburi, Thailand. Recruitment was conducted through posted announcements, and individuals who expressed interest were screened by the researcher according to predefined inclusion and exclusion criteria. Group assignment was determined by recruitment period rather than individual randomization. Participants enrolled during the initial recruitment phase were allocated to the control group, whereas those enrolled during the subsequent phase were assigned to the experimental group. Because participants were not individually randomized, this allocation procedure is consistent with a quasi-experimental design. To minimize contamination between groups, participants in the control and experimental arms were scheduled for follow-up activities at different times.
The first author implemented the self-management program, delivered educational sessions, provided instructional materials, and coordinated follow-up activities through a mobile application under the supervision of CCOP and PP. Participant engagement was monitored throughout the 12-week intervention period, and clarification or adherence support was provided as needed. Pretest and posttest data were collected using a structured electronic questionnaire administered via Google Forms. Baseline assessments were completed during outpatient visits before participants were informed of their group assignment to avoid response bias. Posttest assessments were completed at the 12-week follow-up through Google Forms.
Although participants were aware of their group assignment during posttest data collection, they were instructed not to disclose this information to maintain assessor blinding during data analysis. All clinical outcomes, including eGFR, systolic and DBP, and HbA1c, were obtained using standardized laboratory and automated measurement procedures. These procedures minimized measurement bias and supported the feasibility of maintaining assessor blinding. No protocol deviations occurred during the study. All procedures were conducted in accordance with the approved research protocol and ethical guidelines.
The intervention used in this study was a mobile communication application developed based on the Individual and Family Self-Management Program to slow the progression of CKD. The program was delivered through the LINE chatbot platform, which enabled continuous communication among participants, their family members, and the research team. The chatbot was developed in collaboration with PCOP, who provided technical and clinical consultation in designing the chatbot structure and interactive functions to support self-management activities. Development of the intervention followed the KDIGO guidelines and the clinical practice guidelines of the Nephrology Society of Thailand for slowing kidney deterioration. Educational materials were deliberately designed to be concise, user-friendly, and accessible, using plain language, large fonts, clear typography, intuitive illustrations, and short videos to enhance comprehension and engagement. All content was reviewed by three nephrology nursing specialists and two nephrologists to ensure content validity and clinical accuracy, and revisions were made based on expert feedback and pilot testing prior to implementation.
The intervention was guided by Ryan and Sawin’s IFSMT [22], which emphasizes enhancing knowledge and beliefs, strengthening self-regulation skills, and fostering social facilitation through family engagement to improve self-management behaviors and health outcomes. To operationalize IFSMT within the program, each intervention component was systematically aligned with the theory’s three core constructs. The knowledge and beliefs construct was addressed through structured educational sessions, an electronic self-management manual, and multimedia instructional videos. The self-regulation construct was reinforced through guided goal setting, regular self-monitoring of blood pressure and body weight, monthly behavior-tracking forms, and individualized action plan development. The social facilitation construct was integrated by actively engaging family caregivers in all educational and coaching sessions and by using the LINE chatbot to deliver reminders, enhance motivation, and support ongoing communication among participants, caregivers, and the research team. Collectively, these strategies ensured coherent translation of the theoretical framework into practical implementation of the intervention.
The intervention consisted of four integrated components. First, the self-management manual (e-book) addressed four key topics: blood pressure control, blood sugar control, health behavior modification—including physical activity, weight management, smoking cessation, dietary adjustments, and avoidance of secondhand smoke—and medication adherence. Second, multimedia educational videos were developed to complement the manual. Five short videos addressed blood sugar management, blood pressure management, behavioral and lifestyle modification, dietary recommendations, and medication management, and were embedded within the LINE platform to allow flexible and repeated viewing. Third, the self-management record system, developed using Google Forms, enabled participants to document their self-management behaviors. Participants recorded blood pressure measurements for three consecutive days each month, tracked monthly body weight, and completed a personalized action plan for slowing stage 3 CKD progression, thereby supporting self-monitoring and reflection over time. Finally, educational notification messages were used to reinforce knowledge and support behavior change. Concise messages were delivered three times per week (Monday, Wednesday, and Friday) through the LINE chatbot, with each message addressing a single topic using clear and supportive language to sustain engagement among participants and caregivers.
The intervention was delivered over a 12-week period through five structured sessions, as summarized in Table 1. All sessions were conducted via LINE video calls and the chatbot platform, allowing integration of real-time and asynchronous communication. Session 1 focused on building rapport, collecting baseline data, and orienting participants and caregivers to the digital platform. Session 2 emphasized enhancing knowledge and beliefs related to CKD through interactive discussions and scenario-based analyses. Sessions 3 and 4 focused on developing self-regulation skills, including goal setting, self-monitoring, planning, self-evaluation, and management of emotional and behavioral responses. Session 5 was conducted in week 12 as a follow-up to evaluate changes in self-management behaviors and clinical outcomes. Participants in the control group received standard care, consisting of routine follow-up visits and standard health education provided by the nephrology outpatient clinic. Between scheduled educational sessions, ongoing intervention activities were continuously implemented. Participants recorded their daily self-management behaviors through the LINE chatbot, received educational messages three times per week, and accessed automated chatbot support. The research team monitored adherence and provided follow-up reinforcement as needed. Family members supported daily self-management practices as part of the family-centered approach. Throughout the 12-week program, family members played an active role by participating in all educational and coaching sessions, assisting participants with goal setting, and helping monitor daily self-management behaviors, including medication adherence, dietary control, symptom observation, and blood pressure monitoring. Family members also supported participants in using the LINE chatbot by assisting with data entry and reviewing educational messages. During weeks without scheduled sessions, family members provided ongoing encouragement, reminding participants about necessary health behaviors. This structured involvement was intended to strengthen social support and enhance the sustainability of self-management behaviors.
5. Ethical Considerations
This study was approved by the Institutional Review Board of Burapha University (No. G-HS055/2566) and registered with the Thai Clinical Trials Registry (TCTR20240920001). Participants received detailed information regarding the study objectives, procedures, potential benefits, and their right to decline or withdraw from participation at any time. Written informed consent was obtained prior to data collection. All data were kept confidential and reported in aggregate form only. Research documents and electronic data will be securely destroyed one year after publication of the study findings, with paper records shredded using a cross-cut shredder and electronic files permanently deleted using data-erasure software.
6. Data Analysis
Data were analyzed using IBM SPSS ver. 26 (IBM Corp., Armonk, NY, USA), with statistical significance set at p<.05. Descriptive statistics, including frequency, percentage, mean, and standard deviation, were used to summarize demographic characteristics and baseline health data. Baseline comparisons between experimental and control groups were conducted using the chi-square test and Fisher exact test, as appropriate. Prior to inferential analyses, all dependent variables were assessed for normality using the Shapiro-Wilk test, boxplots, and Q-Q plots. No significant outliers were identified, and assumptions for parametric testing were satisfied. Within-group changes were examined using the paired t-test, while between-group comparisons were conducted using the independent t-test. Analysis of covariance (ANCOVA) was used to adjust for baseline differences. The Levene test confirmed homogeneity of variance (p>.05), and the interaction between group assignment and baseline covariates was not statistically significant (p>.05), indicating parallel regression slopes and confirming the appropriateness of ANCOVA.
RESULTS
1. Demographic Data, Health Information Data, and Homogeneity of Study Sample
A total of 50 participants were enrolled in the study, with 25 assigned to the experimental group and 25 to the control group. In the experimental group, most participants were male (60.0%). The majority were in the middle to late elderly age range, with more than half aged over 70 years (52.0%). Regarding educational attainment, most participants (52.0%) had completed primary school or less. Most participants (68.0%) reported having sufficient income or savings to meet their living expenses. Primary caregiving responsibilities were most commonly provided by relatives (60.0%). In the control group, most participants were female (60.0%). A higher proportion were aged over 70 years compared with the experimental group (80.0%). Educational attainment was generally lower, with 76.0% having completed primary school or less. Most participants (60.0%) indicated that they had sufficient income or savings to support their living expenses. Similarly, most primary caregivers were relatives (72.0%).
In terms of health-related characteristics, participants in the experimental group showed the following clinical profiles: 48.0% were classified as having obesity class I (BMI, 25.00–29.99 kg/m²), and 64.0% were diagnosed with stage 3a CKD, defined by an eGFR of 45–59 mL/min/1.73 m². In addition, 44.0% had HbA1c levels above 7.0%, 68.0% had SBP values greater than 140 mmHg, and 8.0% had DBP values above 90 mmHg. All participants in this group had a diagnosis of hypertension, and 80.0% had comorbid diabetes mellitus and hyperlipidemia. With respect to pharmacologic management, all participants were prescribed antihypertensive medications, 80.0% received antidiabetic agents, 96.0% were receiving lipid-lowering therapy, and 24.0% were prescribed medications for anemia. Among participants in the control group, 40.0% were classified as having obesity class I, and a higher proportion (80.0%) had stage 3a CKD. Forty percent had HbA1c levels above 7.0%, and 72.0% had SBP values exceeding 140 mmHg. Regarding comorbidities, 96.0% were diagnosed with hypertension, 88.0% with diabetes mellitus, and 76.0% with hyperlipidemia. In terms of pharmacologic treatment, 84.0% were prescribed antihypertensive medications, 88.0% received antidiabetic therapy, 80.0% were treated with lipid-lowering agents, and 28.0% received medications for anemia. A summary of health-related characteristics is presented in Table 2.
No statistically significant differences were observed between the experimental and control groups with respect to demographic, socioeconomic, or clinical characteristics at baseline. These findings indicate that the two groups were comparable prior to the intervention.
2. Within-Group Changes in Self-Management Behavior, eGFR, SBP, DBP, and HbA1c in the Intervention and Control Groups from Baseline to Follow-up
Within the experimental group, participation in the self-management program was associated with significant improvements across several outcomes (Table 3). Self-management behavior scores increased significantly (p<.001), and renal function improved, as reflected by a significant increase in eGFR values (p<.05). Significant reductions were also observed in SBP (p<.001) and DBP (p<.05). In contrast, HbA1c levels did not change significantly, indicating that glycemic control remained stable over the 12-week study period. In the control group, self-management behavior scores also showed a statistically significant improvement following receipt of standard care (p<.001). However, renal function declined, as evidenced by a significant reduction in eGFR from baseline to follow-up (p<.001). Both SBP and DBP increased significantly during the study period (SBP, p<.05; DBP, p<.05), indicating worsening blood pressure control under standard care conditions. Glycemic control, assessed using HbA1c, did not change significantly, with the difference between baseline and follow-up remaining non-significant (p=.440).
3. Between-Group Changes in Self-Management Behavior, eGFR, SBP, DBP, and HbA1c in the Intervention and Control Groups from Baseline to Follow-up
Baseline comparisons showed no statistically significant differences between the experimental and control groups in eGFR (p=.278), SBP (p=.231), DBP (p=.611), or HbA1c (p=.973) prior to the intervention (Table 3). A statistically significant difference in self-management behavior scores was observed between groups at baseline (p<.05). Before conducting the ANCOVA, the interaction between group assignment and baseline covariates was examined and found to be non-significant (p>.05), supporting the assumption of parallel regression slopes. After adjustment for baseline values, participation in the Individual and Family Self-Management Program resulted in significant improvements across multiple outcomes (Table 3). Self-management behavior scores increased significantly in the intervention group compared with the control group (F=7.92, p<.05). Renal function, measured by eGFR, also improved significantly (F=52.92, p<.001), indicating a clinically meaningful improvement among participants with stage 3 CKD. Significant reductions in blood pressure were observed in the intervention group, with marked decreases in SBP (F=26.84, p<.001) and DBP (F=12.61, p<.001). Glycemic control, reflected by HbA1c levels, also improved significantly in the intervention group (F=7.74, p<.05). Collectively, these findings demonstrate strengthened self-management behaviors and improvements in key clinical outcomes over the 12-week intervention period. Overall, the results indicate that the Individual and Family Self-Management Program effectively enhanced behavioral outcomes and contributed to improved renal function, blood pressure control, and glycemic regulation among patients with stage 3 CKD.
4. Additional Findings
No adverse events or unintended effects were reported in either group during the study period. Participants actively engaged with the self-management program through a structured recording system. They monitored blood pressure for three consecutive days each month, tracked monthly body weight, and completed individualized action plans designed to slow stage 3 CKD progression. Adherence to these activities was high, with full participation reported (100%). Participants also reported that the mobile communication application was easy to use and facilitated adherence to recommended self-management behaviors through reminders and regular messaging. Most participants indicated that family members actively supported their participation in the program, which contributed to sustained engagement throughout the 12-week intervention period. These findings suggest that the intervention was feasible, usable, and acceptable for patients with stage 3 CKD.
DISCUSSION
This study demonstrated the effectiveness of an Individual and Family Self-Management Program in slowing the progression of stage 3 CKD. Participants in the intervention group showed significant improvements in self-management behavior scores, eGFR, SBP, and DBP compared with both their baseline values and the control group. These findings are consistent with Ryan and Sawin’s IFSMT [22], which proposes that effective self-management emerges through three interrelated process dimensions: knowledge and beliefs, self-regulation skills and abilities, and social facilitation. By integrating these components into the intervention, the program supported adaptive self-management behaviors that translated into meaningful behavioral and clinical improvements.
The results further showed that participants in the intervention group experienced significantly greater improvements in self-management behaviors, renal function (eGFR), blood pressure (SBP and DBP), and HbA1c compared with those in the control group. These between-group differences indicate that the intervention produced effects beyond those expected from natural disease variation or routine outpatient care alone. The magnitude and consistency of improvements in the intervention group align with prior evidence indicating that structured self-management support can strengthen treatment adherence and improve physiological outcomes among patients with stage 3 CKD. In contrast, the control group exhibited minimal improvement or clinical deterioration across several outcomes, underscoring the added value of the intervention.
The knowledge and beliefs component of the intervention was addressed through structured educational sessions delivered via LINE video calls and chatbot-based communication. Participants received evidence-based information through an electronic self-management manual, multimedia materials, and scenario-based learning activities. Reflective exercises were incorporated to help participants identify and correct misconceptions related to CKD progression and self-management. This approach fostered accurate disease-related beliefs and increased confidence in applying knowledge to daily self-care. Consistent with IFSMT, individuals who develop adequate knowledge and positive beliefs are more likely to adopt and sustain effective self-management behaviors, which is supported by the improvements observed in this study.
The intervention also emphasized the development of self-regulation skills, including goal setting, self-monitoring, reflective thinking, decision-making, planning, self-evaluation, and management of behavioral and emotional responses. These skills were practiced through daily self-monitoring of blood pressure, body weight, and health behaviors using Google Form-based tools. Participants worked collaboratively with family caregivers and the research team to address barriers, refine action plans, and support adherence to individualized goals. Strengthening these self-regulation skills enabled participants to manage their health behaviors more effectively in accordance with their clinical status, which likely contributed to improved blood pressure control and preservation of kidney function.
Social facilitation was integrated throughout the program through active engagement of family caregivers and the use of digital communication platforms. Caregivers participated in educational and coaching sessions, provided daily support, and assisted patients in implementing self-management strategies. The LINE chatbot and group video calls functioned as continuous channels for information exchange, reminders, and motivational support. Previous studies have highlighted the importance of family involvement and social support in sustaining self-management among patients with chronic illnesses [29,30]. Consistent with these findings, the combination of family engagement and digital support in this study likely contributed to improvements in both behavioral and physiological outcomes. Although formal mediation analyses were not conducted, the pattern of results aligns with the causal pathways proposed by IFSMT, suggesting that coordinated enhancement of knowledge, self-regulation, and social facilitation underpinned the intervention’s effectiveness.
Notably, no participant attrition occurred during the 12-week follow-up period. This high retention rate may be attributed to the continuous support provided through the mobile communication application, which enabled regular reminders, timely responses to participants’ questions, and sustained engagement with the program. In addition, family involvement in monitoring and supporting self-management behaviors likely enhanced adherence and reduced the likelihood of dropout. Together, these factors contributed to full participation throughout the intervention period.
The findings of this study are consistent with prior research demonstrating the benefits of family-oriented self-management interventions for individuals with chronic conditions. Chamnan et al. [29] reported that an Individual and Family Self-Management Program improved phosphorus control among hemodialysis patients by strengthening knowledge, beliefs, self-regulation skills, and family involvement. Similarly, Vergara Escobar and Carrillo Gonzalez [30] found that a self-management intervention significantly enhanced self-management behaviors, disease knowledge, coping capacity, and the patient–healthcare provider relationship. Collectively, these studies support the effectiveness of IFSMT-guided interventions that target multiple self-management processes simultaneously.
In contrast, the study did not detect a statistically significant difference in HbA1c levels between the intervention and control groups. Several factors may explain this finding. First, data collection occurred between January and May 2024, overlapping with the Songkran Festival, a national holiday period associated with increased social gatherings and less structured dietary practices, which may have influenced dietary adherence. Second, HbA1c reflects average blood glucose levels over approximately 120 days, corresponding to the lifespan of erythrocytes [31], and therefore requires sufficient time to capture meaningful changes [32]. Similar results have been reported in previous studies. Mata and Chiewchantanakit [33] observed improvements in fasting blood glucose but not HbA1c after a 12-week self-efficacy–based intervention in patients with type 2 diabetes, while Kongtong [34] reported no significant HbA1c change following a 3-month family-supervised behavioral modification program among patients with poorly controlled diabetes. These findings suggest that longer intervention durations or extended follow-up periods may be necessary to observe clinically meaningful changes in HbA1c among patients with stage 3 CKD and comorbid diabetes.
Several previous studies have highlighted the importance of family support in improving self-management among patients with chronic diseases. Research in CKD populations has shown that family involvement enhances medication adherence, dietary control, symptom monitoring, and clinic attendance, which in turn leads to improved clinical outcomes. Similar findings have been reported in studies of diabetes and hypertension, where strong family support has been associated with better lifestyle modification and adherence to treatment. These findings align with the IFSMT and support the results of the present study, in which active participation by family members contributed to improvements in self-management behaviors, blood pressure, and eGFR among participants.
Overall, the results provide strong support for the application of IFSMT to self-management interventions in CKD. By simultaneously targeting knowledge and beliefs, self-regulation skills, and social facilitation, the program achieved measurable improvements in both behavioral and clinical outcomes. The integration of digital platforms, including the LINE chatbot, video calls, and online monitoring tools, facilitated continuity of care, accessibility, and sustained engagement. These features are particularly valuable for patients with chronic diseases who face barriers to frequent in-person care. Collectively, these findings underscore the potential of structured, theory-based, digitally supported interventions to enhance patient self-management and slow disease progression.
1. Implications of the Study
This study demonstrates that an Individual and Family Self-Management Program delivered through a mobile communication platform can improve both self-management behaviors and clinical outcomes among patients with stage 3 CKD. Guided by Ryan and Sawin’s IFSMT [22], the program focused on enhancing knowledge and beliefs, strengthening self-regulation skills, and fostering social facilitation through family engagement. As a result, participants showed significant improvements in eGFR, SBP and DBP, and self-management behavior scores, suggesting a slowing of disease progression.
The findings have several important implications. For clinical practice, nurses should integrate structured, theory-based self-management programs into routine care for patients with stage 3 CKD to promote sustained behavior change and improved outcomes. Traditional outpatient consultations often do not provide sufficient time or continuity to support complex lifestyle modifications. In this context, mobile application-based interventions can address these limitations by enabling ongoing communication, reinforcement of self-management behaviors, and active involvement of family members.
For health service administrators and policymakers, implementing IFSMT-based self-management programs for other chronic conditions may improve patient outcomes while optimizing healthcare resource utilization. Such programs should prioritize accessible education, development of behavioral skills, and structured social support mechanisms. These elements can be adapted to different populations and disease contexts, supporting scalable and sustainable approaches to chronic disease management.
For nursing education, integrating training in self-management support, particularly through digital platforms, may better prepare nurses to lead patient- and family-centered interventions. The findings of this study also support the further development of nurse-led digital interventions that extend care beyond traditional clinical settings and enhance continuity of care for patients with chronic illnesses, including stage 3 CKD.
2. Limitations of This Study
The use of mobile applications in patient care may pose challenges for older adults or individuals with limited digital literacy. To support effective implementation, additional assistance may be required to help patients and family members navigate the technology. Differences in familiarity with internet-based activities may also influence engagement and intervention outcomes. Future programs should incorporate pre-intervention assessments of digital readiness and provide tailored training to address these disparities.
CONCLUSION
This study provides evidence that a theory-based Individual and Family Self-Management Program can slow disease progression and improve self-management behaviors and clinical outcomes among patients with stage 3 CKD. Integrating this intervention into routine nursing care represents a practical and effective strategy for patients, families, and healthcare teams. Broader implementation of similar digitally supported programs may contribute to improved chronic disease management and better long-term patient outcomes.
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
AUTHORSHIP
Study conception and/or design acquisition - SK, CCOP, PP, and PCOP; analysis - SK, CCOP, PP, and PCOP; interpretation of the data - SK, CCOP, PP, and PCOP; and drafting or critical revision of the manuscript for important intellectual content - SK and CCOP.
FUNDING
None.
ACKNOWLEDGEMENT
The authors thank all participants who willingly participated in the research activities.
DATA AVAILABILITY STATEMENT
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Figure 1.
CONSORT 2010 flow diagram.
Table 1.
Overview of an Individual and Family Self-Management Program via a Mobile Application
Activities
Time
Materials used
Session 1: week 1 day 1 (face-to-face)
60 minutes
- The personal demographic questionnaires
This initial face-to-face session will focus on establishing rapport and building a therapeutic relationship with participants and their primary caregiver. The session will include:
- The health status questionnaires
- Building rapport through friendly and welcoming interactions.
- Self-management behaviors for slowing CKD progression questionnaires
- Conducting a comprehensive assessment, including the collection of personal information, health status, and current self-management behaviors related to slowing the progression of CKD.
- Multimedia
- Orienting the experimental group and their primary caregiver to the media and equipment that will be utilized throughout the intervention.
- Self-management for slowing CKD progression record
- Exchange experiences and beliefs about CKD, the researcher will reflect on these beliefs to identify misconceptions and provide accurate information.
- Multimedia
- The self-management manual for slowing CKD progression (e-book)
Activity 2: educational activity (video calls)
40–60 minutes
- LINE video call
- Assess knowledge of the experimental group and their primary caregiver after studying the multimedia.
- The self-management manual for slowing CKD progression (e-book)
- Provide example situations for the experimental group and their primary caregiver to jointly analyze how to slow kidney failure progression.
Session 3: week 1 day 3 (video calls)
40–60 minutes
- LINE video call
Activity 3: Self-Management Skills Training, Part 1
- Educational notification message
This session will focus on practical applications of self-management skills.
- Self-management for slowing CKD progression record
- The experimental group will engage in guided practice of key self-management skills, including goal setting, self-monitoring and reflective thinking, decision-making, and action planning related to slowing CKD progression.
- LINE Official Account and Chatbot
- Participants will record their daily self-management behaviors related to slowing CKD progression using a Google Form accessible via the Line chatbot. This daily recording will continue until the end of the program.
- The researcher will send a message via LINE three times a week (Mondays, Wednesdays, and Fridays) with a single topic related to CKD self-management. These messages will continue until the program’s conclusion.
Session 4: week 2 day 3 (video calls)
30 minutes
- Educational notification message
Activity 3: self-management skills training, part 2
- Self-management for slowing CKD progression record
- This session will build upon the skills learned in the previous session and introduce additional self-management techniques.
- LINE Official Account and Chatbot
- The experimental group will practice self-management skills, including self-evaluation and response management related to their CKD.
- Participants will continue to record their daily self-management behaviors related to slowing CKD progression using a Google Form accessible via the Line chatbot. This daily recording will continue until the end of the program.
Session 5: week 12 (face-to-face)
30 minutes
- Self-management behaviors for slowing CKD progression questionnaires
This final face-to-face session will serve as a follow-up assessment after completion of the program. The session will include:
- Post-program evaluation of self-management behaviors related to slowing CKD progression.
- Collection of clinical data, including estimated glomerular filtration rate, systolic blood pressure, diastolic blood pressure, and hemoglobin A1c.
CKD=chronic kidney disease.
Table 2.
Demographic Data, Health Information Data, and Homogeneity of Study Sample (N=50)
Changes in Self-Management Behavior, Estimated Glomerular Filtration Rate, Systolic Blood Pressure, and Diastolic Blood Pressure among the Intervention and Control Groups from Baseline to Follow-up (N=50)
3. Department of Disease Control, Ministry of Public Health. More details of the Ministry of Public Health and fiscal year 2022 [Internet]. Nonthaburi: Department of Disease Control, Ministry of Public Health; 2022 [cited 2025 October 1]. Available from: https://ddc.moph.go.th/uploads/publish/1308820220905025852.pdf
5. Toyama M, Satoh M, Nakayama S, Hashimoto H, Muroya T, Murakami T, et al. Combined effects of blood pressure and glucose status on the risk of chronic kidney disease. Hypertens Res. 2024;47(7):1831-41. https://doi.org/10.1038/s41440-024-01683-x
6. Srina J, Adisuksodsai D. Survival rate and factors affecting mortality in peritoneal dialysis patients, Chumphea Hospital. Nakhon Phanom Hosp J. 2019;6(2):36-45.
7. Silarak T, Piyabunditkul L, Kittipichai W. Predictive factors of chronic kidney disease in patients with diabetes mellitus at Sisaket province. Songklanagarind J Nurs. 2020;40(2):109-21.
10. Hinkhaw C, Hanprasitkam K, Jianvitayakij S. Effects of a combination of self-management and motivational interviewing program for delayed progression of diabetic nephropathy on self-management behaviors and clinical outcomes among type 2 diabetic patients with third-stage diabetic nephropathy. J Phrapokklao Nurs Coll. 2019;30(2):185-202.
11. Ku E, Johansen KL, McCulloch CE. Time-centered approach to understanding risk factors for the progression of CKD. Clin J Am Soc Nephrol. 2018;13(5):693-701. https://doi.org/10.2215/CJN.10360917
12. Jiang Z, Wang Y, Zhao X, Cui H, Han M, Ren X, et al. Obesity and chronic kidney disease. Am J Physiol Endocrinol Metab. 2023;324(1):E24-41. https://doi.org/10.1152/ajpendo.00179.2022
13. Lin CW, Chen IW, Lin YT, Chen HY, Hung SY. Association of unhealthy dietary behaviors with renal function decline in patients with diabetes. BMJ Open Diabetes Res Care. 2020;8(1):e000743. https://doi.org/10.1136/bmjdrc-2019-000743
14. Singhkum S, Chumnanborirak P. Empowering the community health network for improving quality of care for patients with chronic renal disease. Mahasarakham Hosp J. 2019;16(3):149-58.
15. Teemueangsai W, Paksupasin P. Development of delayed chronic kidney disease model in primary CKD clinic, Mueang district, Mahasarakham province. Mahasarakham Hosp J. 2021;18(3):125-35.
16. Chen CH, Lin TM, Hung SC, Wu MJ, Tsai SF. A quality improvement initiative for patients with chronic kidney disease to promote their smoking cessation. Tob Induc Dis. 2023;21:127. https://doi.org/10.18332/tid/170626
17. Lee YJ, Cho S, Kim SR. Effect of alcohol consumption on kidney function: population-based cohort study. Sci Rep. 2021;11(1):2381. https://doi.org/10.1038/s41598-021-81777-5
18. Evangelidis N, Craig J, Bauman A, Manera K, Saglimbene V, Tong A. Lifestyle behaviour change for preventing the progression of chronic kidney disease: a systematic review. BMJ Open. 2019;9(10):e031625. https://doi.org/10.1136/bmjopen-2019-031625
19. Doommai N, Ponpinij P, Moungkum S, Masingboon K. Factors influencing behavior for delaying progression of kidney impairment among patients with chronic kidney disease stage 1–3. Thai Pharm Health Sci J. 2022;17(4):378-85.
20. Yoomuang P, Suphunnakul P. Mobile application for slowing chronic kidney disease progression based on creer self-management. EAU Herit J Sci Technol. 2019;13(3):32-43.
22. Ryan P, Sawin KJ. The individual and family self-management theory: background and perspectives on context, process, and outcomes. Nurs Outlook. 2009;57(4):217-25. https://doi.org/10.1016/j.outlook.2008.10.004
23. Tubart L. The effects of a model slowing the progression of patients with stage 3 chronic kidney disease at Neon Maprang district, Phitsanulok province [master’s thesis]. Nonthaburi: Sukhothai Thammathirat University; 2016.
24. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York: Routledge; 1988.
28. Gray JR, Grove SK. Burns & Grove’s the practice of nursing research: appraisal, synthesis, and generation of evidence. 9th ed. St. Louis, MO: Elsevier; 2021.
29. Chamnan A, Kitsripisarn S, Tasanarong A. Impact of individual and family self-management programme on hemodialysis-treated patients’ adherence to phosphorus control and on their calcium x phosphorus product. J Thai Nurse Midwife Counc. 2021;36(2):49-65.
30. Vergara Escobar OJ, Carrillo Gonzalez GM. Self-management program in adults with colorectal cancer: a pilot study. Aquichan. 2023;23(1):e2317. https://doi.org/10.5294/aqui.2023.23.1.7
31. Obeagu EI. Red blood cells as biomarkers and mediators in complications of diabetes mellitus: a review. Medicine (Baltimore). 2024;103(8):e37265. https://doi.org/10.1097/MD.0000000000037265
32. Evans M, Welsh Z, Seibold A. Reductions in HbA1c with flash glucose monitoring are sustained for up to 24 months: a meta-analysis of 75 real-world observational studies. Diabetes Ther. 2022;13(6):1175-85. https://doi.org/10.1007/s13300-022-01253-9
33. Mata C, Chiewchantanakit D. Effects of self-efficacy-based program in type 2 diabetes mellitus patients with poor glycemic control. Thai Pharm Health Sci J. 2023;18(4):354-60.
34. Kongtong J. The effect of a case study program on behavioral health modification for diabetic patients who cannot control blood sugar level by supervision of their relatives. J Res Health Innov Dev. 2024;5(1):69-78. https://he01.tci-thaijo.org/index.php/jrhi/article/view/268172/180877
The Effects of an Individual and Family Self-Management Program for Slowing Disease Progression via a Mobile Application on Self-Management Behaviors and Clinical Outcomes in Patients with Stage 3 Chronic Kidney Disease in Thailand: A Quasi-Experimental Study
Figure 1. CONSORT 2010 flow diagram.
Figure 1.
The Effects of an Individual and Family Self-Management Program for Slowing Disease Progression via a Mobile Application on Self-Management Behaviors and Clinical Outcomes in Patients with Stage 3 Chronic Kidney Disease in Thailand: A Quasi-Experimental Study
Overview of an Individual and Family Self-Management Program via a Mobile Application
Activities
Time
Materials used
Session 1: week 1 day 1 (face-to-face)
60 minutes
- The personal demographic questionnaires
This initial face-to-face session will focus on establishing rapport and building a therapeutic relationship with participants and their primary caregiver. The session will include:
- The health status questionnaires
- Building rapport through friendly and welcoming interactions.
- Self-management behaviors for slowing CKD progression questionnaires
- Conducting a comprehensive assessment, including the collection of personal information, health status, and current self-management behaviors related to slowing the progression of CKD.
- Multimedia
- Orienting the experimental group and their primary caregiver to the media and equipment that will be utilized throughout the intervention.
- Self-management for slowing CKD progression record
- Exchange experiences and beliefs about CKD, the researcher will reflect on these beliefs to identify misconceptions and provide accurate information.
- Multimedia
- The self-management manual for slowing CKD progression (e-book)
Activity 2: educational activity (video calls)
40–60 minutes
- LINE video call
- Assess knowledge of the experimental group and their primary caregiver after studying the multimedia.
- The self-management manual for slowing CKD progression (e-book)
- Provide example situations for the experimental group and their primary caregiver to jointly analyze how to slow kidney failure progression.
Session 3: week 1 day 3 (video calls)
40–60 minutes
- LINE video call
Activity 3: Self-Management Skills Training, Part 1
- Educational notification message
This session will focus on practical applications of self-management skills.
- Self-management for slowing CKD progression record
- The experimental group will engage in guided practice of key self-management skills, including goal setting, self-monitoring and reflective thinking, decision-making, and action planning related to slowing CKD progression.
- LINE Official Account and Chatbot
- Participants will record their daily self-management behaviors related to slowing CKD progression using a Google Form accessible via the Line chatbot. This daily recording will continue until the end of the program.
- The researcher will send a message via LINE three times a week (Mondays, Wednesdays, and Fridays) with a single topic related to CKD self-management. These messages will continue until the program’s conclusion.
Session 4: week 2 day 3 (video calls)
30 minutes
- Educational notification message
Activity 3: self-management skills training, part 2
- Self-management for slowing CKD progression record
- This session will build upon the skills learned in the previous session and introduce additional self-management techniques.
- LINE Official Account and Chatbot
- The experimental group will practice self-management skills, including self-evaluation and response management related to their CKD.
- Participants will continue to record their daily self-management behaviors related to slowing CKD progression using a Google Form accessible via the Line chatbot. This daily recording will continue until the end of the program.
Session 5: week 12 (face-to-face)
30 minutes
- Self-management behaviors for slowing CKD progression questionnaires
This final face-to-face session will serve as a follow-up assessment after completion of the program. The session will include:
- Post-program evaluation of self-management behaviors related to slowing CKD progression.
- Collection of clinical data, including estimated glomerular filtration rate, systolic blood pressure, diastolic blood pressure, and hemoglobin A1c.
Self-management behaviors for slowing CKD progression scores
2.41±0.30
2.71±0.15
2.28±0.19
2.55±0.18
6.15 (<.001)
6.34 (<.001)
1.82 (<.05)
3.45 (.001)
7.92 (.007)
Estimated glomerular filtration rate
48.06±6.16
51.14±7.04
49.59±5.23
44.18±4.74
3.00 (.006)
–10.42 (<.001)
–0.95 (.278)
4.10 (<.001)
52.92 (<.001)
Systolic blood pressure
144.64±13.00
132.24±11.81
138±17.37
145.36±14.55
–4.74 (<.001)
2.73 (<.05)
1.53 (.231)
–3.50 (.001)
26.84 (<.001)
Diastolic blood pressure
74.92±12.13
70.08±8.91
70.00±11.59
76.40±12.53
–2.48 (.021)
3.01 (<.05)
1.47 (.611)
–2.06 (.045)
12.61 (<.001)
Hemoglobin A1c
6.92±1.78
6.64±1.30
7.06±1.72
7.19±1.37
1.89 (.072)
0.78 (.440)
–0.28 (.973)
–1.46 (.150)
7.74 (.008)
Table 1. Overview of an Individual and Family Self-Management Program via a Mobile Application
CKD=chronic kidney disease.
Table 2. Demographic Data, Health Information Data, and Homogeneity of Study Sample (N=50)
BMI=body mass index;
Fisher’s exact test.
Table 3. Changes in Self-Management Behavior, Estimated Glomerular Filtration Rate, Systolic Blood Pressure, and Diastolic Blood Pressure among the Intervention and Control Groups from Baseline to Follow-up (N=50)


 E-SUBMISSION
E-SUBMISSION