Abstract
-
Purpose
Inadequate bowel preparation compromises the efficacy of colonoscopy. This study aimed to develop and evaluate a patient-tailored bowel preparation program designed to improve bowel preparation quality, medication adherence, and dietary adherence among patients undergoing colonoscopy.
-
Methods
The program consisted of four phases: (1) patient-specific assessment using a checklist; (2) personalized instructional videos; (3) short message service reminders; and (4) nurse-led counseling. A quasi-experimental, nonconcurrent nonequivalent control group, posttest-only design was used, with the control group recruited first. The study was conducted from April to July 2024 at a tertiary hospital in South Korea and included 80 adult outpatients scheduled for colonoscopy (40 control and 40 experimental participants). Outcomes included bowel preparation quality assessed using the Aronchick Bowel Preparation Scale, medication knowledge and adherence, and dietary knowledge and adherence.
-
Results
The experimental group demonstrated significantly higher bowel preparation quality than the control group (Z=8.13, p<.001, r=0.91). Medication knowledge and adherence were also significantly higher in the experimental group than in the control group (Z=3.54, p<.001, r=0.40; Z=6.50, p<.001, r=0.73; respectively). Similarly, dietary knowledge and adherence improved significantly in the experimental group compared with the control group (Z=5.28, p<.001, r=0.59; Z=5.32, p<.001, r=0.60; respectively).
-
Conclusion
The patient-tailored bowel preparation program effectively improved bowel preparation outcomes for colonoscopy. Future research should focus on integrating the program into electronic health records to enable automated delivery and improve efficiency and scalability in clinical practice.
-
Key Words: Patient-centered care; Colonoscopy; Laxatives; Nursing care
INTRODUCTION
As one of the leading causes of cancer-related mortality, colorectal cancer requires effective screening strategies, with colonoscopy considered the most reliable method for early detection and prevention [
1,
2]. Colonoscopy is regarded as the gold standard for colorectal cancer screening because it enables not only the early detection of malignancies but also the removal of precancerous adenomas before malignant transformation occurs [
1,
2]. In addition, colonoscopy facilitates therapeutic interventions, such as hemostasis for lower gastrointestinal bleeding, further underscoring its diagnostic and therapeutic value [
3]. However, the effectiveness of colonoscopy depends heavily on adequate bowel preparation because inadequate cleansing impairs mucosal visualization, prolongs procedure time, increases complication risk, and reduces the adenoma detection rate by up to 20% [
4]. Recognizing these implications, the U.S. Multi-Society Task Force recommends adequate bowel preparation in at least 85% of procedures, whereas European guidelines recommend a higher benchmark of 90%, both assessed using validated scales [
5,
6]. Therefore, optimizing bowel preparation is essential for ensuring the diagnostic accuracy and overall effectiveness of colonoscopy.
Although adequate bowel preparation is essential for successful colonoscopy, the reported rate of inadequate bowel cleansing ranges from 16.9% to 50.0% [
7]. Several factors contribute to inadequate preparation, including sociodemographic characteristics such as older age, male sex, and obesity, as well as medical conditions including inpatient status, constipation, liver disease, hypertension, diabetes, and stroke [
7]. A recent prospective study identified male sex, diabetes, constipation, previous colorectal surgery, consumption of a high-fiber diet within 24 hours before colonoscopy, and a bowel preparation-to-procedure interval exceeding 5 hours as independent risk factors for inadequate bowel preparation [
8]. These findings highlight the importance of patient-tailored approaches that account for individual medical conditions and age-related factors to improve bowel preparation efficacy and overall colonoscopy outcomes. In Korean clinical settings, suboptimal bowel preparation has been reported in approximately one-third of colonoscopies, with older age and comorbidity burden identified as major contributing factors, further supporting the need for risk-informed educational support [
9].
Systematic reviews have identified several interventions aimed at improving bowel preparation quality, including paper-based educational materials, video-based education, and telephone-based re-education [
10,
11]. More recently, technology-based approaches, such as mobile applications and virtual reality, have been explored as innovative strategies to improve bowel cleansing efficacy [
12]. However, printed materials typically provide standardized content without accounting for patient-specific characteristics, such as age or comorbidities [
13], whereas technology-based education may be less accessible to older adults, who represent a substantial proportion of patients undergoing colonoscopy [
14]. South Korean intervention studies have similarly reported benefits from reinforced education delivered near key preparation milestones. For example, telephone- or short message service (SMS)-based re-education shortly before colonoscopy improved bowel preparation quality compared with usual instruction [
15]. In nursing-led education studies, patient educational video programs improved knowledge, adherence, and bowel cleanliness [
16]. Collectively, these previous approaches were largely limited to single-modality interventions and did not systematically integrate risk stratification with multimodal reinforcement throughout the preprocedural period, highlighting the need for a more structured patient-tailored program.
Given these limitations, there is an increasing need for patient-tailored bowel preparation education that accounts for individual factors, including age, underlying medical conditions, bowel preparation agents, and recommended split-dose regimens [
17]. Recent studies have demonstrated the effectiveness of personalized educational interventions in which specialized nurses tailor educational content according to patients’ health literacy, medical history, prescribed medications, and age [
18]. These tailored interventions have shown superior outcomes in bowel preparation quality and adherence compared with conventional approaches [
18]. Building on this evidence, the present study aimed to develop a patient-tailored bowel preparation program (PTBPP) and evaluate its effectiveness. The primary outcome was bowel preparation quality. Secondary outcomes included patients’ knowledge of and adherence to bowel preparation medications, as well as their knowledge of and adherence to dietary recommendations related to bowel preparation.
METHODS
1. Development and Configuration of the PTBPP
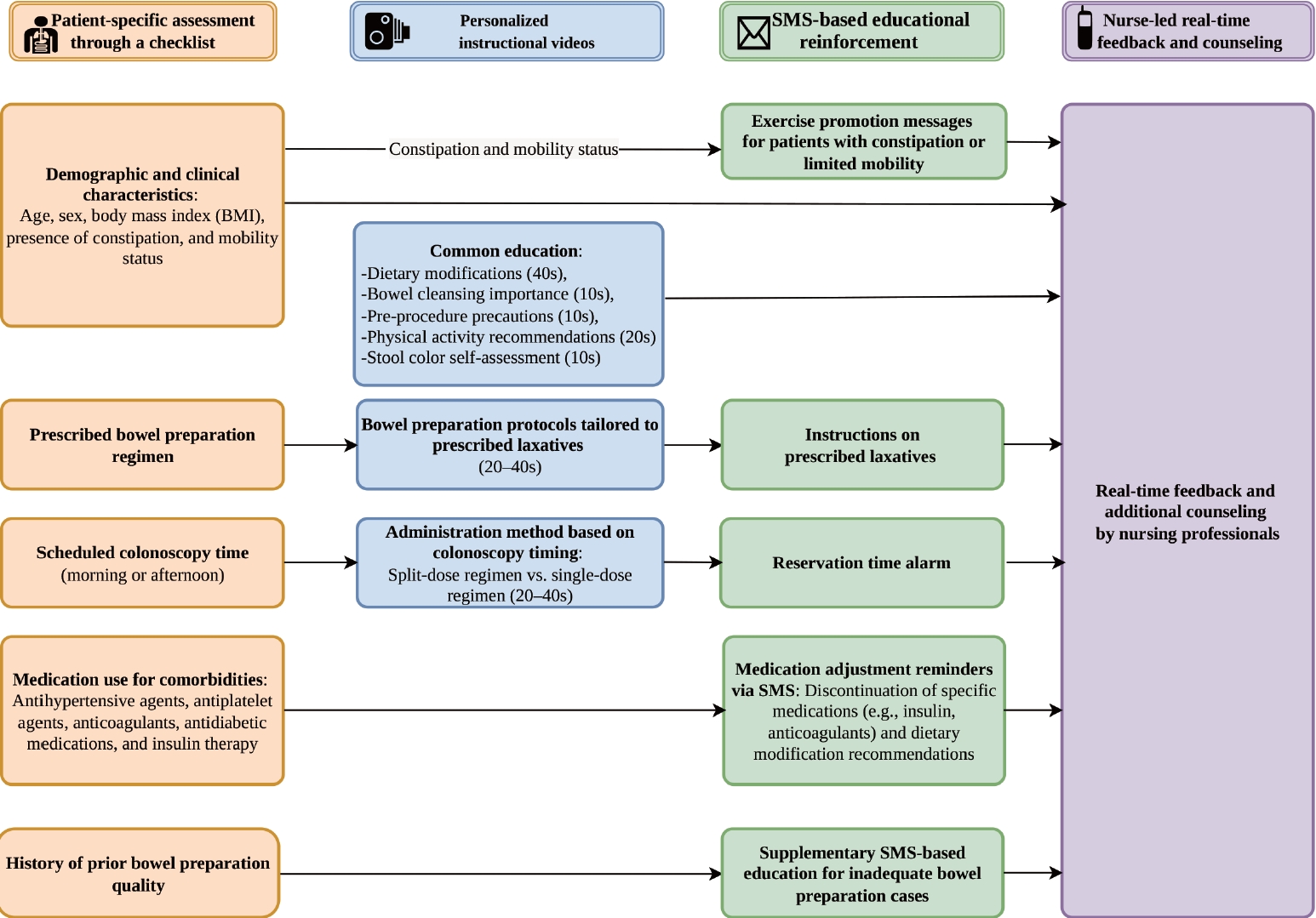
The PTBPP was developed as a four-phase intervention to optimize colonoscopy preparation through patient-specific assessment, personalized instructional videos, SMS reminders, and real-time nurse-led counseling [
6].
1) Development process and expert validation
The content of this tailored framework was based on a comprehensive literature review. Searches were conducted in PubMed, Google Scholar, and RISS, identifying five systematic reviews and guidelines [
6,
19-
22] and one reference textbook [
23]. The PTBPP clinical protocols were aligned with the European Society of Gastrointestinal Endoscopy (ESGE) 2019 guidelines and the Korean Guidelines for Postpolypectomy Colonoscopic Surveillance (2022) to ensure regional clinical relevance and safety within the Korean medical context.
The content validity of the preliminary program was evaluated by a panel of five experts, including three gastroenterologists and two endoscopy nurses, using a 4-point Likert scale. Validation included 26 items across three domains: (1) the patient-specific assessment checklist (10 items); (2) personalized instructional videos (8 items); and (3) SMS-based educational reinforcement (8 items). The Item-Content Validity Index (I-CVI) ranged from 0.80 to 1.00 across all domains, and the overall Scale-level Content Validity Index (S-CVI/Ave) was 0.96, indicating high content validity.
Based on expert feedback, the medication-management instructions were revised by replacing the fixed cessation period for antithrombotic agents with a requirement for mandatory confirmation from the prescribing physician to prevent clinical complications. In addition, the timing of counseling phone calls was advanced from 1 day before to 2 days before the procedure, ensuring that patients had sufficient time for dietary adjustment and bowel preparation.
2) Final configuration of the PTBPP
The final PTBPP was structured around an operational logic that systematically linked individual assessment data to subsequent intervention components, ensuring that all educational content and counseling were aligned with each participant’s clinical profile (
Figure 1).
(1) Phase 1: patient-specific assessment through a checklist
The first phase involved developing a pre-colonoscopy checklist to identify individual patient characteristics and clinical risk factors, including age, bowel habits, mobility, comorbidities, and previous experiences [
6]. These assessment results served as the primary input data for customizing the subsequent phases. Specifically, a predefined mapping logic was applied: the prescribed agent and procedure timing determined the video selection in phase 2; chronic constipation or a history of inadequate preparation triggered intensified SMS reinforcement in phase 3; and individual risk factors provided the basis for phase 4 telephone counseling. The detailed operational mapping of these variables to each intervention component is presented in
Supplementary Table 1.
(2) Phase 2: personalized instructional videos
The second phase involved developing and disseminating personalized educational videos tailored to individual patient characteristics [
10]. The PTBPP included seven video modules: five standardized educational videos and two individualized videos. The standardized videos covered the importance of bowel cleansing, dietary modifications, medications requiring special precautions, physical activity recommendations after bowel preparation, and stool color self-assessment to determine bowel cleansing adequacy. The individualized videos provided bowel preparation instructions according to the prescribed bowel cleansing agent and colonoscopy timing (morning vs. afternoon), ensuring that patients received an appropriate split-dose or single-dose regimen.
The video guides for bowel preparation regimens were tailored according to the prescribed laxative type and scheduled colonoscopy time and ranged from 20 to 40 seconds. The common educational videos, which addressed dietary modifications and general bowel preparation guidelines, ranged from 10 to 40 seconds. Each participant received a personalized set of seven videos with a total duration of 2 minutes to 3 minutes 40 seconds.
(3) Phase 3: SMS-based educational reinforcement
The third phase focused on improving adherence through personalized SMS reminders [
15]. Text messages were tailored to each patient’s prescribed bowel preparation agent, scheduled colonoscopy time, and comorbid conditions. These messages included medication-specific instructions; guidance on discontinuing antihypertensive agents, antidiabetic medications, anticoagulants, and antiplatelet drugs; and insulin suspension protocols. Personalized SMS reminders were delivered beginning 7 days before colonoscopy, with each participant receiving 2 to 3 messages during this period. Patients with a history of inadequate bowel preparation also received supplementary SMS reminders with tailored bowel-cleansing instructions to improve adherence.
(4) Phase 4: nurse-led real-time feedback and counseling
The fourth phase involved real-time feedback and individualized counseling conducted by an experienced endoscopy nurse via telephone 2 days before the procedure [
24]. Using a standardized counseling and assessment sheet derived from the phase 1 checklist data, the nurse verified adherence to the bowel preparation protocol and provided individualized guidance. This guidance included confirmation of the prescribed laxative regimen, including timing and dosage; verification of medication adjustments for comorbidities, such as antihypertensive, antidiabetic, and insulin therapies, with mandatory physician confirmation for antithrombotic cessation; reinforcement of dietary restrictions; and intensified support for high-risk patients, including those with chronic constipation or a history of inadequate preparation (
Supplementary Table 1). Active listening techniques were used to address patient concerns and enhance engagement.
1) Study design
This study used a quasi-experimental, nonconcurrent nonequivalent control group, posttest-only design to evaluate the effects of the PTBPP on bowel preparation quality, knowledge of and adherence to laxatives, and dietary knowledge and adherence (
Supplementary Figure 1). Because the control group was recruited and assessed first, followed by the intervention group, this nonconcurrent design was used to minimize contamination.
Three hypotheses were tested. First, patients who participated in the PTBPP were hypothesized to demonstrate significantly different bowel preparation quality compared with those who received usual paper-based education (hypothesis 1). Second, patients who participated in the PTBPP were hypothesized to demonstrate significantly different knowledge of and adherence to bowel preparation medications compared with those who received usual paper-based education (hypothesis 2). Third, patients who participated in the PTBPP were hypothesized to demonstrate significantly different knowledge of and adherence to dietary recommendations for bowel preparation compared with those who received usual paper-based education (hypothesis 3).
Participants in both groups received a standardized explanation of the overall study procedures for bowel preparation education and colonoscopy. However, they were not explicitly informed of their assigned study group, namely, usual paper-based education or the PTBPP.
2) Setting and participants
This study was conducted from April to July 2024 at a 1,130-bed tertiary teaching hospital in Gwangju, South Korea. Participants were recruited from the gastroenterology outpatient clinic among patients scheduled for colonoscopy during the study period. Eligible participants were adults aged 19 years or older who were scheduled to undergo colonoscopy. The exclusion criteria were as follows: (1) diagnosed psychiatric disorder; (2) documented cognitive impairment, such as dementia or delirium, or communication difficulties that precluded informed consent or completion of study procedures; and (3) inability to complete any component of the PTBPP.
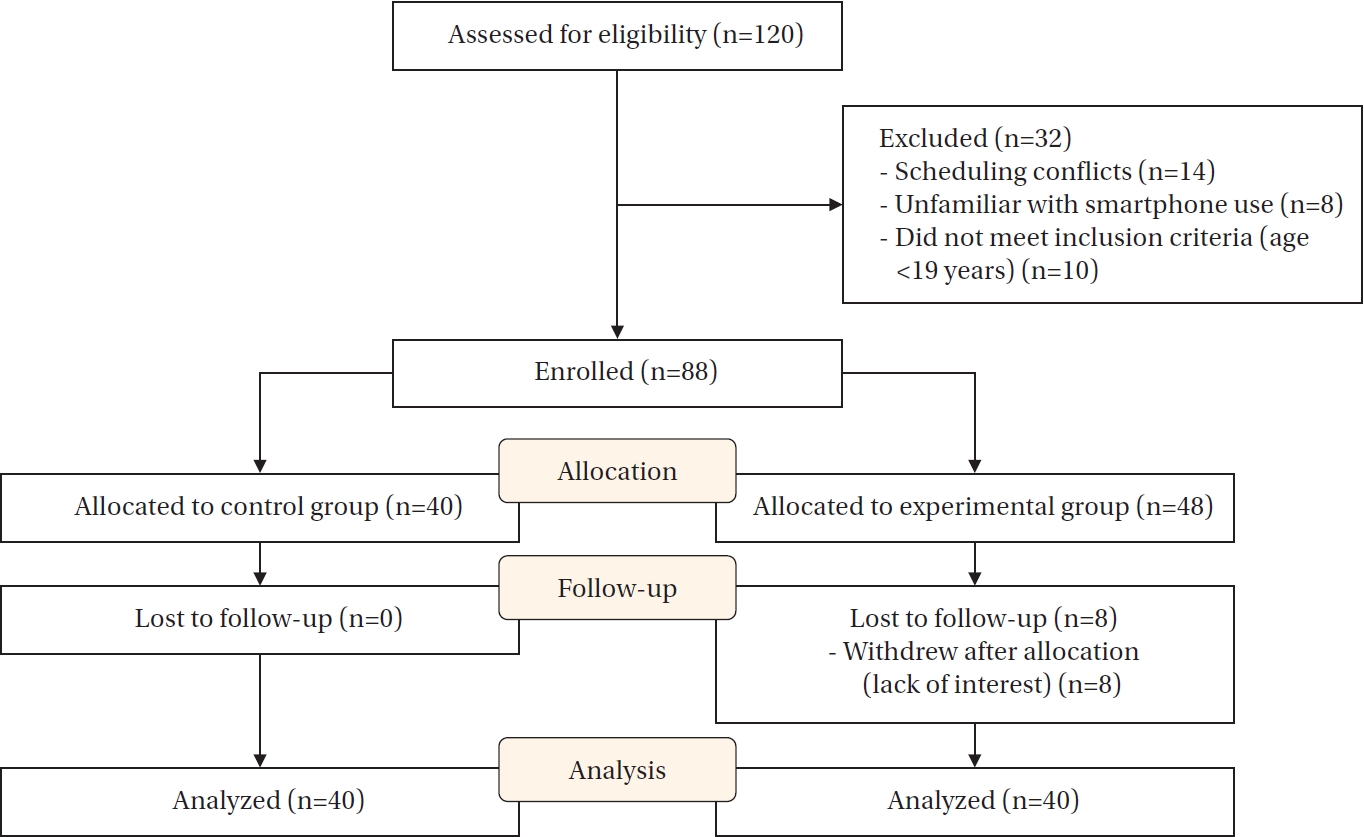
The sample size was calculated using G*Power 3.1.9.7 (Heinrich Heine University Dusseldorf, Dusseldorf, Germany). An a priori power analysis was conducted using the Wilcoxon-Mann-Whitney test. Based on the meta-analytic effect size (d=0.66) of educational video interventions [
10], 80% statistical power, and a two-tailed significance level of 5%, the required sample size was 76 participants (38 per group). To accommodate an estimated dropout rate of approximately 15%, the final target sample size was set at 88 participants.
A total of 120 participants were screened for eligibility. Thirty-two were not enrolled: 10 did not meet the inclusion criterion of age ≥19 years, 14 had scheduling conflicts, and eight had difficulty using a smartphone. After eligibility assessment, 40 participants were allocated to the control group and 48 to the experimental group. In the experimental group, 8 participants withdrew after allocation because of lack of interest, resulting in 40 participants who completed the study and were included in the analysis (
Figure 2).
3) Measurements/instruments
Bowel-preparation–related baseline variables were selected a priori with reference to the 2019 ESGE guideline update [
6], and demographic characteristics were collected as routine baseline information.
Bowel cleansing quality was assessed using the Aronchick Bowel Preparation Scale (ABPS), a validated tool recommended by the U.S. Multi-Society Task Force on Colorectal Cancer for evaluating bowel preparation adequacy [
5,
25]. The ABPS categorizes bowel preparation into five levels: excellent (5 points), good, fair, poor, and inadequate (1 point), with higher scores indicating better bowel cleansing quality. Assessments were conducted independently by three board-certified endoscopists, each with more than 5 years of experience and performing 5 to 7 procedures daily, who were blinded to group allocation. To ensure inter-rater consistency, the evaluators conducted a calibration session beforehand using representative clinical images for each ABPS category.
Patient knowledge of and adherence to bowel preparation medications were measured using instruments adapted from Yu [
26]. Knowledge was assessed using a five-item true/false questionnaire evaluating understanding of total dosage, mixing instructions, and ingestion speed; each correct response received 2 points and each incorrect response received 1 point, yielding a score range of 5 to 10. Adherence was measured using a five-item scale with a 4-point Likert scale ranging from 1 ("not at all") to 4 ("fully"), with a score range of 5 to 20. Although the original instruments by Yu [
26] did not include initial validity or reliability data, previous research reported high reliability, with Cronbach's α values of .92 for knowledge and .80 for adherence. To reflect current practice and specific laxatives, such as Coolprep and Orafang, the items were updated and content validation was performed by a panel of five experts, including three gastroenterologists and two nurses. The resulting CVI was 0.96 for knowledge and 1.00 for adherence. In this study, the Kuder-Richardson Formula 20 (KR-20) was 0.72 for knowledge, and Cronbach's α was .65 for adherence.
Dietary preparation was assessed using six-item scales adapted from Yu [
26]. The dietary knowledge scale measured participants’ understanding of restrictions on seeded fruits, high-fiber vegetables, whole grains, and seaweed for 3 days before colonoscopy, as well as the requirements for a soft diet and appropriate fasting timing on the day before the procedure. Scoring followed the 2/1-point system, with a score range of 6 to 12. Dietary adherence was evaluated using a six-item, 4-point Likert scale, with total scores ranging from 6 to 24. Validity and reliability were confirmed by a five-expert panel, including three gastroenterologists and two nurses, confirmed the alignment of the items with the 2022 Korean Guidelines; therefore, no modifications were required. Choi and Choi [
27] reported Cronbach’s α values of .84 for dietary knowledge and .80 for adherence. In this study, the KR-20 for dietary knowledge was 0.67, and Cronbach’s α for adherence was .77.
4) Data collection
To prevent intervention contamination, participants were recruited sequentially, with the control group enrolled first and the experimental group enrolled afterward. After Institutional Review Board (IRB) approval and administrative permission from the nursing department and endoscopy unit were obtained, the first author screened eligible patients using the colonoscopy appointment list in the electronic health records (EHRs), according to the inclusion and exclusion criteria, and consecutively approached eligible outpatients. Eligible patients were approached at the time of colonoscopy scheduling or before the procedure, received an explanation of the study, and provided written informed consent before enrollment. Group allocation was determined by recruitment period rather than randomization, with the control group recruited from April to May 2024 and the experimental group recruited from June to July 2024. At scheduling, both groups received the hospital’s standard printed bowel preparation leaflet once in person from a pharmacist at Chonnam National University Hospital. The leaflet included dietary precautions, foods to avoid, instructions on the timing and method of the prescribed bowel preparation agent, and key precautions regarding medication use, with no differences according to colonoscopy appointment time.
All data were collected by the first author, who screened eligibility, reviewed EHRs using a structured checklist, and distributed and collected the self-administered questionnaires. During April–May 2024, the control group received only the printed materials and had no additional contacts. No additional intervention components, including videos, SMS reminders, or telephone counseling, were provided to the control group. During June to July 2024, the experimental group received the PTBPP in addition to the same printed materials. This included personalized instructional videos viewed 8 days before colonoscopy, SMS reminders beginning 7 days before colonoscopy, and a standardized telephone consultation conducted 2 days before the procedure by the first author, an experienced endoscopy nurse with at least 10 years of experience in bowel preparation education. The personalized instructional videos comprised seven short modules with a total duration of 2 minutes to 3 minutes 40 seconds, and SMS reminders were delivered 2 to 3 times according to the tailored schedule. The telephone consultation followed a standardized counseling and assessment sheet to confirm adherence and address barriers. All participants completed self-administered questionnaires measuring bowel preparation knowledge and adherence before the procedure. During colonoscopy, a board-certified endoscopist evaluated bowel preparation quality.
5) Ethical considerations
This study was approved by the IRB of Chonnam National University Hospital (No. CNUH-2024-116). All participants were informed that participation was voluntary, that they could withdraw at any time without consequences, and that anonymity and confidentiality would be maintained. Written informed consent was obtained from all participants. As a token of appreciation, participants received a South Korean Won 5,000 gift for participating. All study data will be stored securely for 3 years and then permanently destroyed. This study was prospectively registered with the Clinical Research Information Service, Republic of Korea, a World Health Organization International Clinical Trials Registry Platform Primary Registry (No. KCT0011066).
6) Data analysis
All data were analyzed using IBM SPSS ver. 29 (IBM Corp., Armonk, NY, USA), with the two-tailed significance level set at 5%. Descriptive statistics, including frequencies, percentages, medians, and interquartile ranges, were used to summarize demographic and baseline characteristics. Normality was assessed using the Shapiro-Wilk test. Because the normality assumption was not met, group homogeneity and between-group differences were assessed using the chi-square test for categorical variables and the Mann-Whitney U test for ordinal or continuous variables.
RESULTS
1. Baseline Characteristics and Homogeneity between Groups
Baseline characteristics were comparable between groups (
Table 1). The homogeneity test showed no significant between-group differences in baseline characteristics, including age, sex, body mass index, education level, presence of underlying diseases, history of colon cancer, previous abdominal surgery, self-administration of bowel preparation medication, constipation, previous colonoscopy experience, and type of laxative (
Table 1).
1) Hypothesis 1 (primary outcome)
Bowel preparation quality was assessed using the ABPS. The experimental group had a significantly higher proportion of “excellent” bowel preparation scores than the control group (95% vs. 5%). In contrast, 85% of participants in the control group were rated as “fair.” The Mann-Whitney U test showed a significant between-group difference (Z=8.13,
p<.001, r=0.91) (
Table 2). Thus, hypothesis 1 was supported.
2) Hypothesis 2 (secondary outcomes)
The experimental group demonstrated significantly higher knowledge of and adherence to bowel preparation medications than the control group. Medication-related knowledge was significantly greater in the experimental group than in the control group (Z=3.54,
p<.001, r=0.40) (
Table 3). Medication adherence was also significantly higher in the experimental group (Z=6.50,
p<.001, r=0.73). Thus, hypothesis 2 was supported.
3) Hypothesis 3 (secondary outcomes)
The experimental group also demonstrated significantly higher knowledge of and adherence to dietary recommendations than the control group. Knowledge of dietary recommendations was significantly greater in the experimental group than in the control group (Z=5.28, p<.001, r=0.59). Adherence to dietary recommendations was also significantly higher in the experimental group (Z=5.32, p<.001, r=0.60). Thus, hypothesis 3 was supported.
DISCUSSION
To strengthen the intervention evaluation, contamination was minimized through sequential recruitment, and assessment bias was reduced through blinded ABPS ratings supported by a prior calibration session. The methodological novelty of this study lies in the development and evaluation of a PTBPP that integrated evidence-based educational strategies, including video-based learning, into a personalized intervention framework. Previous meta-analytic findings demonstrated the effectiveness of video-based education for improving bowel preparation, with an effect size of 0.66 compared with conventional education methods [
10]. Building on this evidence, this study developed a customized PTBPP that included personalized video content tailored to each patient’s prescribed bowel preparation agent and scheduled colonoscopy time. The program was further reinforced through individualized counseling to enhance patient adherence. The effectiveness of this four-phase, patient-tailored, multicomponent approach was confirmed, indicating a large effect [
28]. Together, these findings suggest that embedding validated educational modalities within a structured, patient-specific delivery pathway may produce clinically meaningful improvements beyond conventional education.
Several mechanisms may explain why the PTBPP outperformed previously reported personalized education interventions. First, the PTBPP begins with structured risk stratification using clinical and behavioral predictors, including previous inadequate preparation, constipation, comorbidities, medication profile, and anticipated adherence barriers; this enables early identification of high-risk patients and proactive intensification of support. Second, the PTBPP uses multiple delivery modes and repeated reinforcement, including written materials, structured counseling, and reinforcement contacts, to minimize misinterpretation and improve regimen fidelity. This approach is supported by a randomized trial showing that multimodal patient education can improve bowel preparation outcomes compared with usual care [
29]. Third, the PTBPP incorporates timely reinforcement contacts, such as telephone-based instructions, aligned with key preparation milestones to reduce common implementation failures, including incomplete intake, timing confusion, and misunderstanding of instructions [
24]. Collectively, these components extend beyond information tailoring alone by operationalizing a barrier-responsive, time-sensitive adherence support strategy across the preprocedural timeline.
A key component of this study was the incorporation of multiple personalized intervention methods, including demographic and medical history screening, tailored educational materials, and real-time support. Recent studies of personalized bowel preparation interventions have emphasized the importance of accounting for patient-specific factors, such as age, physical condition, psychological state, and education level, primarily through nurse counseling [
18] or SMS reminders [
15]. In these studies, the reported effect sizes were an odds ratio of 2.090 (Cohen’s d=0.407, medium effect) for bowel preparation quality and an odds ratio of 2.752 (Cohen’s d=0.674, medium-to-large effect) for adherence to bowel preparation medications [
18]. In contrast to these predominantly single-modality approaches, the PTBPP combined risk-informed tailoring with structured, repeated reinforcement across the preparation period, which may have increased implementation fidelity and reduced adherence failures in routine practice. Thus, the present findings support the interpretation that personalization may be most effective when paired with multimodal reinforcement and barrier-responsive support rather than information tailoring alone.
The primary outcome, bowel preparation quality, was assessed using the ABPS, a validated and widely used assessment tool in South Korea [
30]. A survey-based study of 1,032 South Korean participants found that 63.6% achieved an “excellent” or “good” ABPS rating [
30]. Similarly, a study using personalized telephone-based education reported an “excellent/good” rate of 62% [
17]. In contrast, the present study demonstrated superior outcomes, with 95% of participants achieving an “excellent” rating and the remaining 5% classified as “good.” These findings support the effectiveness of the PTBPP and indicate its potential to improve bowel preparation quality compared with conventional personalized education approaches.
In this study, the PTBPP significantly improved medication- and diet-related knowledge and adherence, which are key targets of enhanced patient instructions recommended in bowel preparation guidelines [
6]. Video-based education has been shown to improve bowel preparation outcomes, supporting the use of tailored educational videos to strengthen patients’ understanding of preparation steps [
10]. Reinforced education delivered near the time of colonoscopy via telephone or SMS has been effective in improving bowel preparation quality, suggesting that time-aligned reminders may help translate knowledge into adherence [
15]. A recent meta-analysis also demonstrated that telephone instructions significantly improve bowel preparation quality, supporting nurse-led telephone consultation as a practical strategy for reinforcing medication and dietary instructions [
24]. Multifaceted, person-centered interventions that include active discussion are more likely to improve health literacy and related health behaviors, which may explain the observed gains in knowledge and adherence [
31].
Given the effectiveness of the PTBPP, integration into clinical workflows is an important next step [
32]. This study used EHRs for risk factor screening, allowing efficient identification of high-risk patients. Future work should integrate the PTBPP into EHR systems to enable automated delivery of tailored video education and personalized text messages, thereby reducing the need for manual intervention. Although nurse expertise is essential to the success of personalized interventions, the limited availability of highly skilled healthcare professionals may challenge the scalability of individualized interventions. With advances in artificial intelligence (AI), future research could develop AI-enabled decision support systems that use EHR-derived factors to predict patients at high risk of inadequate bowel preparation and support preprocedural detection or triage to trigger timely rescue instructions [
33]. Such systems may automate routine guidance and reminders while allowing nurses to focus on complex counseling and safety checks [
34].
This study had several limitations. First, because of the nonequivalent control group posttest-only design, baseline knowledge and adherence were not statistically compared. This design was chosen because assessing knowledge of specific laxatives and dietary protocols before education is provided is not practically feasible in clinical settings. In addition, this design eliminated potential pretest sensitization. Although direct baseline measures were not available, the two groups were homogeneous in major clinical and demographic variables. Second, although the primary outcome, bowel preparation quality, was assessed using the ABPS by three endoscopy specialists, inter-rater reliability among the three evaluators was not formally validated. To mitigate this limitation, the evaluators conducted a calibration session beforehand using representative clinical images. The ABPS has been established as a validated tool in previous research [
25], and the expertise of the endoscopists, each with more than 5 years of clinical experience, likely strengthened the validity of the primary outcome assessment. Third, medication- and diet-related knowledge and adherence were measured using self-administered instruments. Although content validity was assessed and internal consistency was examined, further psychometric validation, such as construct validity, criterion validity, and test–retest reliability, was not performed. Fourth, although this study screened multiple risk factors for inadequate bowel preparation and incorporated them into a structured checklist, health literacy was not included in the screening process. Given that health literacy is an important determinant of the effectiveness of personalized interventions [
31], future research should develop comprehensive screening checklists that include literacy assessments to optimize the personalization of educational interventions. Fifth, the intervention effect size may have been overestimated because older adults with limited smartphone proficiency were excluded. Because the intervention required participants to access personalized videos and text messages, eight individuals who had difficulty using mobile phones were excluded. In addition, another eight participants dropped out before completing the study, potentially because of challenges accessing personalized digital content. Therefore, future research should develop programs based solely on telephone counseling for individuals with low digital literacy to ensure more inclusive intervention strategies.
CONCLUSION
This study demonstrated that the PTBPP, which integrated personalized education through videos, SMS reminders, and nurse counseling, significantly improved bowel preparation quality, medication adherence, and dietary adherence compared with conventional paper-based education. Future research should focus on automating the PTBPP within EHR systems and exploring alternative delivery methods, such as telephone-based counseling, to address digital literacy barriers. These findings highlight the need for scalable, AI-assisted personalized interventions to optimize patient education and bowel preparation outcomes in clinical practice.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and design acquisition - SHJ and SHM; data collection - SHJ; data analysis - SHJ; the interpretation of the data - SHJ and SHM; discussion and conclusions - SHJ and SHM; drafting and critical revision of the manuscript - SHJ and SHM.
-
Funding
This work was conducted with the support of the 2024 Health Fellowship Foundation.
-
ACKNOWLEDGEMENT
None.
-
DATA AVAILABILITY STATEMENT
The data can be obtained from the corresponding authors.
SUPPLEMENTARY MATERIAL
Figure 1.Configuration of the patient-tailored bowel preparation program. SMS=short message service.
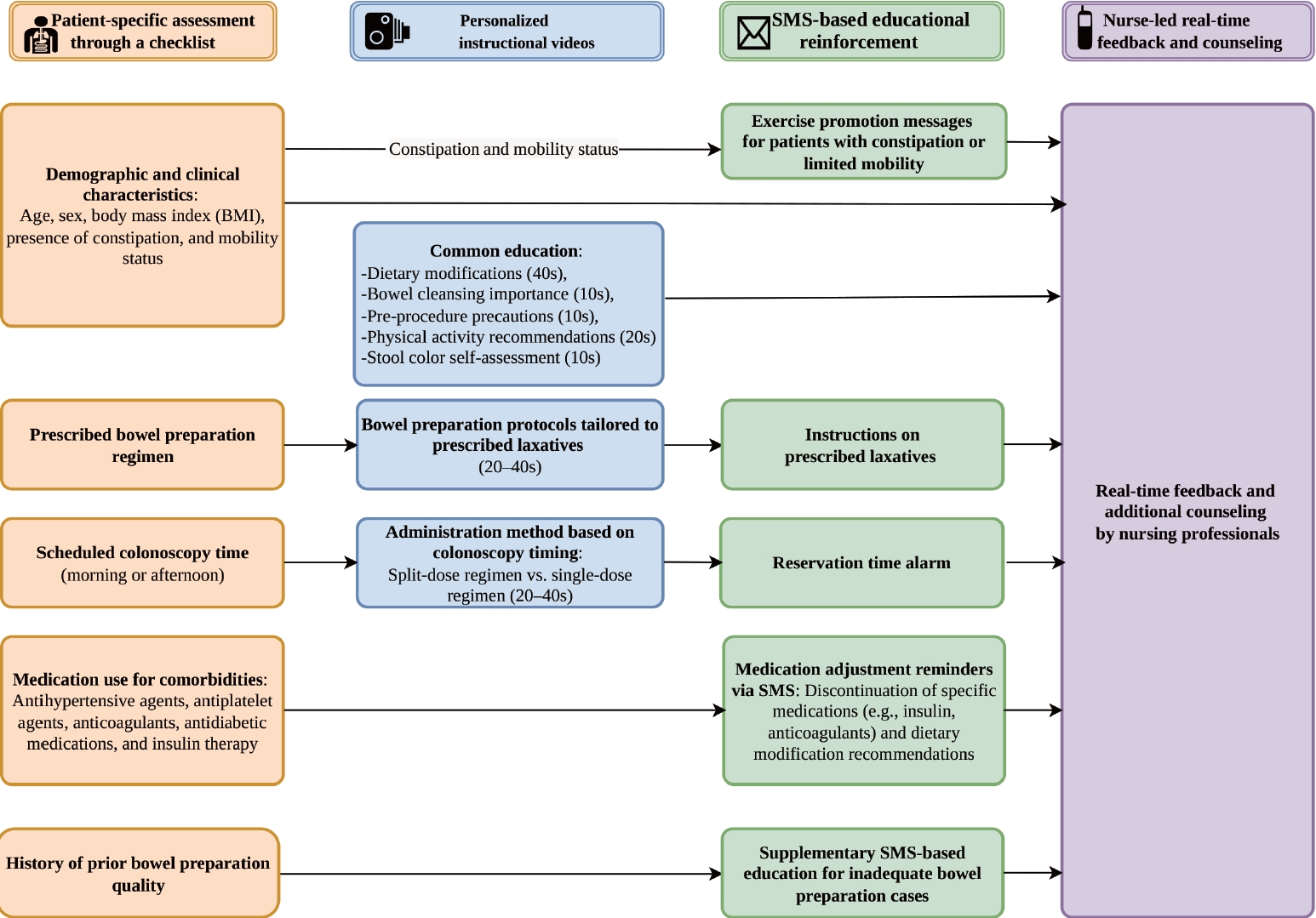
Figure 2.Flow diagram of participants through the study.

Table 1.Baseline Characteristics and Homogeneity between Groups
|
Variables |
Categories |
Total (N=80) |
Control group (n=40) |
Experimental group (n=40) |
χ² or Z |
p
|
|
Median (IQR) or n (%) |
|
Age (year) |
|
59.0 (43.3–69.0) |
63.5 (44.3–72.8) |
52.5 (42.3–66.0) |
–1.29 |
.197 |
|
Sex |
Male |
44 (55.0) |
25 (62.5) |
19 (47.5) |
1.81 |
.178 |
|
Female |
36 (45.0) |
15 (37.5) |
21 (52.5) |
|
Body mass index (kg/m2) |
|
23.6 (22.2–24.9) |
23.5 (21.8–24.6) |
24.1 (22.4–25.7) |
–1.02 |
.310 |
|
Education (year) |
|
14.5 (9.0–16.0) |
14.0 (9.0–16.0) |
15.5 (9.8–16.0) |
–0.54 |
.588 |
|
No. of underlying diseases |
≥1 |
58 (72.5) |
31 (77.5) |
27 (67.5) |
1.00 |
.317 |
|
None |
22 (27.5) |
9 (22.5) |
13 (32.5) |
|
Colon cancer |
Yes |
13 (16.2) |
6 (15.0) |
7 (17.5) |
0.09 |
.762 |
|
No |
67 (83.8) |
34 (85.0) |
33 (82.5) |
|
History of abdominal surgery |
Yes |
35 (43.7) |
17 (42.5) |
18 (45.0) |
0.05 |
.822 |
|
No |
45 (56.3) |
23 (57.5) |
22 (55.0) |
|
Self-administering bowel preparation medication |
Yes |
74 (92.5) |
38 (95.0) |
36 (90.0) |
0.72 |
.396 |
|
No |
6 (7.5) |
2 (5.0) |
4 (10.0) |
|
Constipation |
Yes |
8 (10.0) |
5 (12.5) |
3 (7.5) |
0.56 |
.456 |
|
No |
72 (90.0) |
35 (87.5) |
37 (92.5) |
|
Previous colonoscopy experience |
Yes |
78 (97.5) |
39 (97.5) |
39 (97.5) |
0.00 |
>.999 |
|
No |
2 (2.5) |
1 (2.5) |
1 (2.5) |
|
Type of laxative |
Coolprep |
53 (66.3) |
25 (62.5) |
28 (70.0) |
2.79 |
.425 |
|
SafePrep |
12 (15.0) |
8 (20.0) |
4 (10.0) |
|
Colyte |
1 (1.3) |
1 (2.5) |
0 (0) |
|
Orafang |
14 (17.5) |
6 (15.0) |
8 (20.0) |
Table 2.Comparison of Bowel Preparation Quality Based on the Aronchick Bowel Preparation Scale between Groups
|
Variables |
Total (N=80) |
Control group (n=40) |
Experimental group (n=40) |
U |
Z |
p
|
Effect size (r) |
|
n (%) |
|
Excellent |
40 (50.0) |
2 (5.0) |
38 (95.0) |
45.0 |
8.13 |
<.001 |
0.91 |
|
Good |
5 (6.3) |
3 (7.5) |
2 (5.0) |
|
Fair |
34 (42.5) |
34 (85.0) |
0 (0) |
|
Poor |
1 (1.3) |
1 (2.5) |
0 (0) |
|
Inadequate |
0 (0) |
0 (0) |
0 (0) |
Table 3.Comparison of Knowledge and Adherence to Bowel Preparation between Groups
|
Categories |
Score range |
Total (N=80) |
Control group (n=40) |
Experimental group (n=40) |
U |
Z |
p
|
Effect size (r) |
|
Median (IQR) |
|
Knowledge of bowel preparation medications |
5–10 |
10.0 (10.0–10.0) |
10.0 (9.0–10.0) |
10.0 (10.0–10.0) |
557.0 |
3.54 |
<.001 |
0.40 |
|
Adherence to bowel preparation medications |
5–20 |
19.0 (16.0–20.0) |
16.0 (14.0–18.0) |
20.0 (19.0–20.0) |
145.0 |
6.50 |
<.001 |
0.73 |
|
Knowledge of dietary recommendations |
6–12 |
12.0 (11.0–12.0) |
11.0 (11.0–12.0) |
12.0 (12.0–12.0) |
313.0 |
5.28 |
<.001 |
0.59 |
|
Adherence to dietary recommendations |
6–24 |
23.0 (21.0–24.0) |
22.0 (19.0–23.0) |
24.0 (24.0–24.0) |
281.5 |
5.32 |
<.001 |
0.60 |
REFERENCES
- 1. World Health Organization (WHO). Colorectal cancer [Internet]. Geneva: WHO; 2023 [cited 2025 February 25]. Available from: https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer
- 2. Bretthauer M, Loberg M, Wieszczy P, Kalager M, Emilsson L, Garborg K, et al. Effect of colonoscopy screening on risks of colorectal cancer and related death. N Engl J Med. 2022;387(17):1547-56. https://doi.org/10.1056/NEJMoa2208375
- 3. Gangwani MK, Aziz A, Dahiya DS, Nawras M, Aziz M, Inamdar S. History of colonoscopy and technological advances: a narrative review. Transl Gastroenterol Hepatol. 2023;8:18. https://doi.org/10.21037/tgh-23-4
- 4. Sharma P, Burke CA, Johnson DA, Cash BD. The importance of colonoscopy bowel preparation for the detection of colorectal lesions and colorectal cancer prevention. Endosc Int Open. 2020;8(5):E673-83. https://doi.org/10.1055/a-1127-3144
- 5. Johnson DA, Barkun AN, Cohen LB, Dominitz JA, Kaltenbach T, Martel M, et al. Optimizing adequacy of bowel cleansing for colonoscopy: recommendations from the US multi-society task force on colorectal cancer. Am J Gastroenterol. 2014;109(10):1528-45. https://doi.org/10.1038/ajg.2014.272
- 6. Hassan C, East J, Radaelli F, Spada C, Benamouzig R, Bisschops R, et al. Bowel preparation for colonoscopy: European Society of Gastrointestinal Endoscopy (ESGE) guideline–update 2019. Endoscopy. 2019;51(8):775-94. https://doi.org/10.1055/a-0959-0505
- 7. Zhang Y, Wang L, Wu W, Zhang S, Zhang M, She W, et al. Predictors of inadequate bowel preparation in older patients undergoing colonoscopy: a systematic review and meta-analysis. Int J Nurs Stud. 2024;149:104631. https://doi.org/10.1016/j.ijnurstu.2023.104631
- 8. Yin H, Wang Y, Wang H, Li T, Xu X, Li F, et al. Derivation and validation of a prediction model for inadequate bowel preparation in Chinese outpatients. Sci Rep. 2025;15(1):1430. https://doi.org/10.1038/s41598-025-85816-3
- 9. Woo DH, Kim KO, Jeong DE, Nam YJ, Lee SH, Jang BI, et al. Prospective analysis of factors associated with inadequate bowel preparation for colonoscopy in actual clinical practice. Intest Res. 2018;16(2):293-8. https://doi.org/10.5217/ir.2018.16.2.293
- 10. Ye Z, Chen J, Xuan Z, Gao M, Yang H. Educational video improves bowel preparation in patients undergoing colonoscopy: a systematic review and meta-analysis. Ann Palliat Med. 2020;9(3):671-80. https://doi.org/10.21037/apm.2020.03.33
- 11. Kurlander JE, Sondhi AR, Waljee AK, Menees SB, Connell CM, Schoenfeld PS, et al. How efficacious are patient education interventions to improve bowel preparation for colonoscopy? A systematic review. PLoS One. 2016;11(10):e0164442. https://doi.org/10.1371/journal.pone.0164442
- 12. Gaina MA, Szalontay AS, Stefanescu G, Balan GG, Ghiciuc CM, Bolos A, et al. State-of-the-art review on immersive virtual reality interventions for colonoscopy-induced anxiety and pain. J Clin Med. 2022;11(6):1670. https://doi.org/10.3390/jcm11061670
- 13. Giguere A, Zomahoun HT, Carmichael PH, Uwizeye CB, Legare F, Grimshaw JM, et al. Printed educational materials: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2020;8(8):CD004398. https://doi.org/10.1002/14651858.CD004398.pub
- 14. van der Kruk SR, Zielinski R, MacDougall H, Hughes-Barton D, Gunn KM. Virtual reality as a patient education tool in healthcare: a scoping review. Patient Educ Couns. 2022;105(7):1928-42. https://doi.org/10.1016/j.pec.2022.02.005
- 15. Lee YJ, Kim ES, Choi JH, Lee KI, Park KS, Cho KB, et al. Impact of reinforced education by telephone and short message service on the quality of bowel preparation: a randomized controlled study. Endoscopy. 2015;47(11):1018-27. https://doi.org/10.1055/s-0034-1392406
- 16. Cho YY, Kim HO. Effects of a patient educational video program on bowel preparation prior to colonoscopy. J Korean Acad Nurs. 2015;45(5):704-12. https://doi.org/10.4040/jkan.2015.45.5.704
- 17. Elvas L, Brito D, Areia M, Carvalho R, Alves S, Saraiva S, et al. Impact of personalised patient education on bowel preparation for colonoscopy: prospective randomised controlled trial. GE Port J Gastroenterol. 2017;24(1):22-30. https://doi.org/10.1159/000450594
- 18. Lu L, Huang H. Impact of personalized nursing care on bowel preparation for colonoscopy. J Nurs Care Qual. 2025;40(2):E17-23. https://doi.org/10.1097/NCQ.0000000000000836
- 19. Kim SY, Kwak MS, Yoon SM, Jung Y, Kim JW, Boo SJ, et al. Korean guidelines for postpolypectomy colonoscopic surveillance: 2022 revised edition. Korean J Gastroenterol. 2022;80(3):115-34. https://doi.org/10.4166/kjg.2022.103
- 20. Na JE, Kim ER. How to choose the optimal bowel preparation regimen for colonoscopy. Ewha Med J. 2021;44(4):122-32. https://doi.org/10.12771/emj.2021.44.4.122
- 21. Migaly J, Bafford AC, Francone TD, Gaertner WB, Eskicioglu C, Bordeianou L, et al. The American Society of Colon and Rectal Surgeons clinical practice guidelines for the use of bowel preparation in elective colon and rectal surgery. Dis Colon Rectum. 2019;62(1):3-8. https://doi.org/10.1097/DCR.0000000000001238
- 22. Chirila A, Nguyen ME, Tinmouth J, Halperin IJ. Preparing for colonoscopy in people with diabetes: a review with suggestions for clinical practice. J Can Assoc Gastroenterol. 2022;6(1):26-36. https://doi.org/10.1093/jcag/gwac035
- 23. Anderson ED. Getting a colonoscopy: your guide to preparation, a pain-free procedure, and peace of mind. Bornincredible; 2023.
- 24. He X, Lei X, Li J, Li P. Telephone instructions improve the quality of bowel preparation for colonoscopy: a meta-analysis of randomized controlled trials. PLoS One. 2023;18(11):e0289063. https://doi.org/10.1371/journal.pone.0289063
- 25. Jacobson BC, Calderwood AH. Measuring bowel preparation adequacy in colonoscopy-based research: review of key considerations. Gastrointest Endosc. 2020;91(2):248-56. https://doi.org/10.1016/j.gie.2019.09.031
- 26. Yu SS. The effect of educational booklet on the compliance of bowel preparation for colonoscopy. J KSGNA. 2013;21(2):172-84.
- 27. Choi MH, Song JA. Effects of video assisted education using smartphone on bowel preparation for colonoscopy. J Korean Acad Fundam Nurs. 2017;24(1):60-71. https://doi.org/10.7739/jkafn.2017.24.1.60
- 28. Cohen J. Statistical power analysis for the behavioral sciences. New York, NY: Routledge; 2013.
- 29. Hattab M, Shakhshir M, Khalil C, Mletat R, Rabi R, Yassin R, et al. Multimodal patient education improves bowel preparation for colonoscopy: a randomized controlled trial. BMC Gastroenterol. 2025;26(1):54. https://doi.org/10.1186/s12876-025-04569-5
- 30. Park JH, Kim SJ, Hyun JH, Han KS, Kim BC, Hong CW, et al. Correlation between bowel preparation and the adenoma detection rate in screening colonoscopy. Ann Coloproctol. 2017;33(3):93-8. https://doi.org/10.3393/ac.2017.33.3.93
- 31. Stormacq C, Wosinski J, Boillat E, Van den Broucke S. Effects of health literacy interventions on health-related outcomes in socioeconomically disadvantaged adults living in the community: a systematic review. JBI Evid Synth. 2020;18(7):1389-469. https://doi.org/10.11124/JBISRIR-D-18-00023
- 32. Borosund E, Ruland CM, Moore S, Ekstedt M. Nurses’ experiences of using an interactive tailored patient assessment tool one year past implementation. Int J Med Inform. 2014;83(7):e23-34. https://doi.org/10.1016/j.ijmedinf.2013.10.010
- 33. Gimeno-Garcia AZ, Benitez-Zafra F, Nicolas-Perez D, Hernandez-Guerra M. Colon bowel preparation in the era of artificial intelligence: Is there potential for enhancing colon bowel cleansing? Medicina (Kaunas). 2023;59(10):1834. https://doi.org/10.3390/medicina59101834
- 34. Rony MK, Kayesh I, Bala SD, Akter F, Parvin MR. Artificial intelligence in future nursing care: Exploring perspectives of nursing professionals: a descriptive qualitative study. Heliyon. 2024;10(4):e25718. https://doi.org/10.1016/j.heliyon.2024.e25718


 E-SUBMISSION
E-SUBMISSION
