
| Panicha Ponpinij | 2 Articles |
Purpose
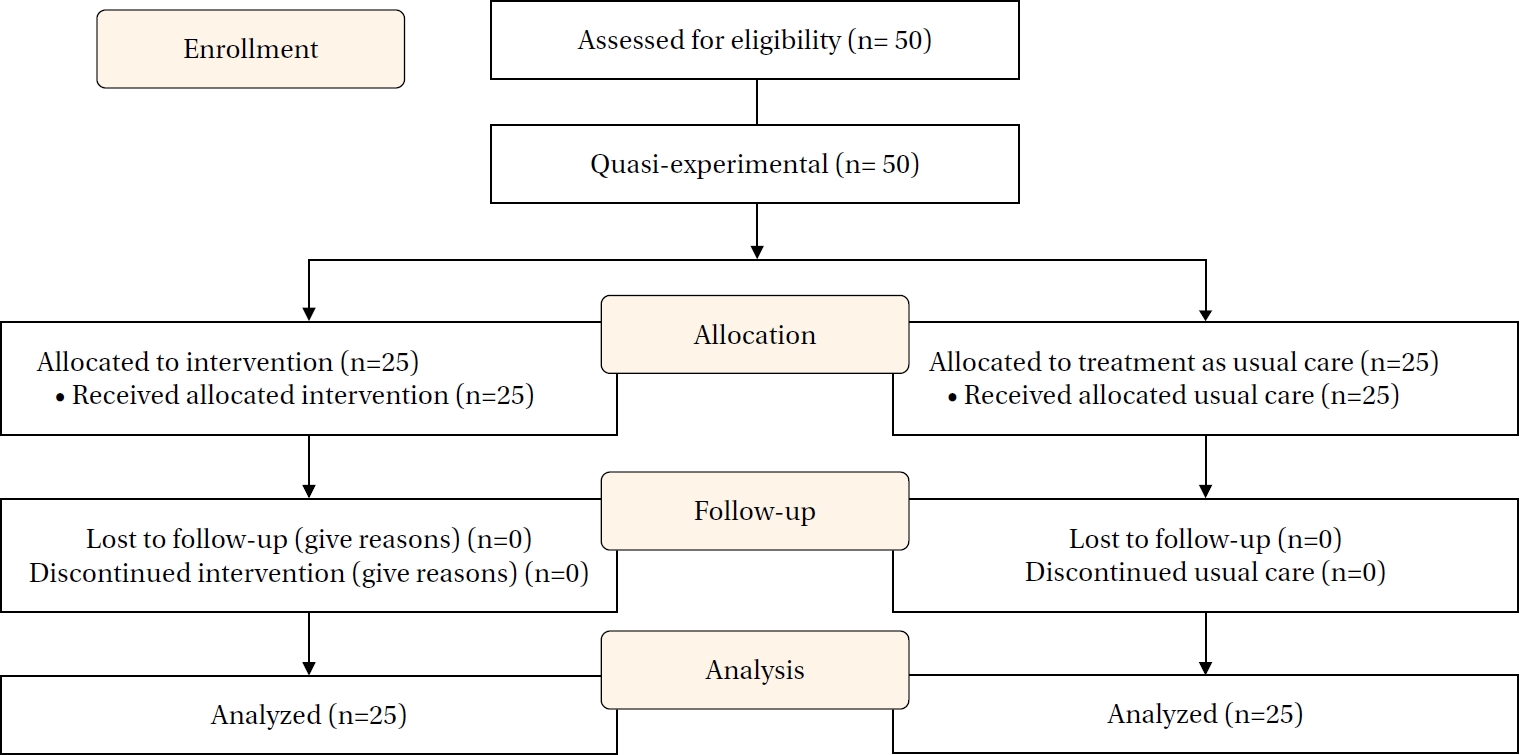
Stage 3 chronic kidney disease (CKD) is highly prevalent and often progresses to end-stage renal disease without effective self-management. This study examined the effects of an Individual and Family Self-Management Program delivered via a mobile communication application on self-management behaviors and clinical outcomes among patients with stage 3 CKD. Methods A 12-week quasi-experimental study with a pretest-posttest control group design was conducted among 50 patients with stage 3 CKD at a tertiary hospital in Thailand, between January and May 2024. The intervention group received a self-management program grounded in Individual and Family Self-Management Theory and delivered via the LINE chatbot. The program included educational content, self-regulation strategies, and structured family support, while the control group received usual care. Outcomes included self-management behaviors, estimated glomerular filtration rate (eGFR), systolic blood pressure (SBP), diastolic blood pressure (DBP), and hemoglobin A1c (HbA1c). Analysis of covariance was used to adjust for baseline differences. Results After adjustment for baseline values, the intervention group showed significantly greater improvements in self-management behaviors (F=7.92, p<.05) and eGFR (F=52.92, p<.001) compared with the control group. Significant reductions were also observed in SBP (F=26.84, p<.001), DBP (F=12.61, p<.05), and HbA1c levels (F=7.74, p<.05). Conclusion A mobile-based Individual and Family Self-Management Program effectively improved self-management behaviors and key clinical outcomes among patients with stage 3 CKD, supporting the integration of family engagement and digital technology in chronic disease care.
Purpose
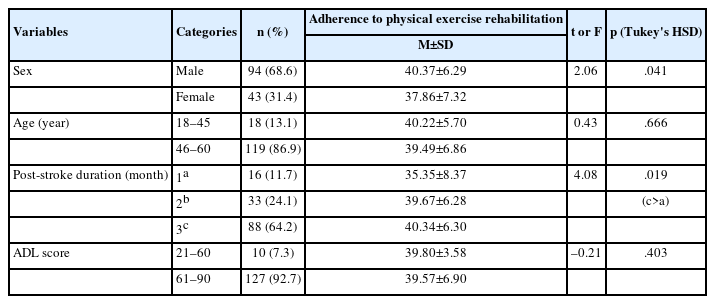
This study aimed to identify key predictive factors influencing adherence to physical exercise rehabilitation among adults during the first three months following a first-onset ischemic stroke in China. Methods: A cross-sectional descriptive study was conducted among 137 adults who attended clinical follow-up appointments within the first three months after experiencing a first-onset ischemic stroke. Predictors included family support, coping with role transition, depression, self-efficacy, and body image. Hierarchical multiple regression analysis was performed. Results: The mean adherence score for physical exercise rehabilitation was 39.58 (standard deviation=6.71), indicating a moderate adherence level (70.6%). In model 1, male sex (β=.20, p=.017) and post-stroke duration of 2 months (β=.31, p=.015) and 3 months (β=.39, p=.002) were significant predictors of adherence to physical exercise rehabilitation. Adding main predictors in model 2 resulted in a significant increase in explained variance (ΔR²=.418, p<.001), accounting for 51.5% of the total variance (R²=.515, adjusted R²=.484). Male sex (β=.15, p=.017), family support (β=.43, p<.001), self-efficacy (β=.26, p<.001), depression (β=–.24, p=.001), and coping with role transition (β=.16, p=.033) were significant predictors. Body image and post-stroke duration were not significant after adjustment. Conclusion: Efforts to promote adherence to physical exercise rehabilitation should prioritize family support, depressive symptoms, self-efficacy, and coping with role transition. Furthermore, body image may warrant attention when developing sex-specific intervention strategies.
|
|
 E-SUBMISSION
E-SUBMISSION