Abstract
-
Purpose
This study examined the association between family functioning and environmental mastery among breast cancer survivors. Specifically, it tested a serial mediation model involving autonomous motivation and healthy behaviors and compared this pathway with the potential role of controlled motivation.
-
Methods
A cross-sectional survey was conducted with 192 community-dwelling Korean breast cancer survivors recruited from an outpatient breast clinic. Participants completed a structured self-administered questionnaire assessing family functioning, autonomous and controlled motivation for self-management, engagement in healthy behaviors, and environmental mastery. Serial mediation was tested using a regression-based bootstrapping approach implemented with Hayes’ PROCESS macro.
-
Results
Family functioning was positively associated with both healthy behaviors and environmental mastery. The serial indirect effect through autonomous motivation and healthy behaviors was significant (standardized indirect effect, 0.03; 95% bootstrapped confidence interval [BootCI], 0.00–0.06). In addition, healthy behaviors independently mediated the association between family functioning and environmental mastery (standardized indirect effect, 0.11; 95% BootCI, 0.05–0.17). Controlled motivation was not significantly associated with family functioning and did not contribute to indirect effects.
-
Conclusion
Supportive family functioning may enhance environmental mastery primarily through greater engagement in healthy behaviors, including a significant sequential pathway involving autonomous motivation. These findings support family-centered, autonomy-supportive approaches that strengthen healthy behaviors to promote psychological adjustment during breast cancer survivorship.
-
Key Words: Breast neoplasms; Family relations; Health behavior; Psychological adaptation; Motivation
INTRODUCTION
Breast cancer has a high survival rate, with 5-year survival rates now approaching 90% to 91% in many high-income settings, reflecting substantial advances in early detection and treatment [
1,
2]. Breast cancer survivors frequently face long-term survivorship demands, including persistent treatment-related symptoms (e.g., fatigue, pain, lymphedema), hormonal therapy-related side effects, body image concerns, and ongoing follow-up care, while simultaneously resuming family and work roles [
2]. Environmental mastery, one of the key dimensions of psychological well-being proposed by Ryff [
3], refers to the perceived competence to manage life demands, utilize available resources, and shape one’s circumstances in accordance with personal values and goals. Within the survivorship context, it represents an important indicator of positive psychosocial adaptation [
4]. Despite its conceptual relevance, survivorship research has primarily focused on adverse outcomes such as distress and functional impairment, with comparatively less attention devoted to positive adaptation outcomes, including environmental mastery.
Emerging evidence suggests that environmental mastery may be strengthened through sustained engagement in healthy behaviors and supportive interpersonal relationships [
4-
6]. Engagement in healthy behaviors has been positively associated with environmental mastery, reflecting an increased perceived capacity to manage daily demands and life circumstances [
4,
5]. Within the cancer survivorship literature, physical activity has been linked to enhanced bodily control and empowerment, which may facilitate broader psychosocial adjustment during recovery [
4,
6]. Identifying modifiable psychosocial and behavioral pathways that contribute to environmental mastery may therefore inform survivorship care aimed at enhancing daily functioning and long-term quality of life.
Family is a primary source of support for cancer survivors, and family functioning has been identified as a critical determinant of quality of life across multiple domains among families affected by cancer, with effects that may persist as the disease progresses [
7,
8]. Among breast cancer patients specifically, supportive family functioning characterized by high cohesiveness and expressiveness has been associated with lower psychological distress, whereas conflictual family patterns predict higher levels of depression and anxiety [
8,
9]. Consistent evidence from breast cancer and broader survivorship research indicates that supportive family functioning is associated with better adjustment and quality of life, whereas conflictual or disengaged family environments are linked to poorer outcomes [
7-
9]. Nevertheless, the mechanisms linking family functioning to survivors’ environmental mastery—defined as the perceived ability to manage and reshape one’s environment during survivorship—remain insufficiently understood.
Self-determination theory (SDT) provides a useful framework for explaining how family functioning shapes motivation and, in turn, behavioral and psychosocial outcomes [
10]. According to SDT, the quality of motivation underlying behavior can be differentiated into autonomous and controlled forms, depending on whether actions reflect personal values and volition or external pressures, guilt, and contingent rewards [
11,
12]. Motivational quality is closely linked to the satisfaction of three basic psychological needs—autonomy, competence, and relatedness [
12,
13]—and family functioning represents an important interpersonal context that can either support or undermine these needs. Adaptive family functioning may support survivors’ psychological needs and autonomous motivation by fostering involvement, shared decision-making, and open communication [
8-
10,
14,
15]. In contrast, family environments characterized by high conflict and poor problem-solving may undermine need satisfaction and strengthen controlled motivation driven by pressure, obligation, or fear of disappointing family members [
8,
10]. Accordingly, family functioning can be viewed as a key contextual factor shaping motivational quality and, consequently, an upstream determinant of survivors’ healthy behaviors and environmental mastery.
Healthy behaviors are essential for maintaining physical and psychological health throughout cancer survivorship [
16]. Active engagement in behaviors such as regular exercise, healthy eating, and stress management may enhance environmental mastery by increasing perceived control over one’s health and daily life [
12,
13]. A substantial body of research highlights the importance of supportive family functioning in the adoption and maintenance of healthy behaviors [
17,
18]. In addition, several studies have reported associations between both autonomous and controlled forms of motivation and engagement in healthy behaviors and related health outcomes [
12,
13,
16]. However, although controlled motivation may prompt short-term behavior change, it often shows limited sustainability and may negatively affect long-term well-being. It therefore remains unclear whether, and to what extent, these motivational processes account for the association between supportive family functioning and survivors’ environmental mastery.
Cancer survivorship requires substantial environmental mastery, as survivors must manage ongoing health needs, navigate complex medical systems, and reorganize daily routines while coping with persistent treatment effects. Despite these theoretical links, few studies of breast cancer survivors have simultaneously examined the sequential pathway from family functioning through motivation and subsequent healthy behaviors to environmental mastery, leaving the psychosocial and behavioral mechanisms underlying this positive adaptation outcome insufficiently specified. The present study therefore examined whether motivation (autonomous and controlled) and healthy behaviors explain the association between family functioning and environmental mastery among breast cancer survivors. Consistent with SDT’s proposition that motivation influences sustained behavioral engagement and, through this pathway, broader psychological well-being and development, we tested a sequential mediation model in which motivation relates to healthy behaviors, which in turn relate to environmental mastery as a positive adaptation outcome.
METHODS
1. Research Design
This study used a cross-sectional descriptive design to examine the dual mediating roles of motivation (autonomous and controlled) and healthy behaviors in the association between family functioning and environmental mastery among breast cancer survivors. This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
2. Setting and Samples
In cancer survivorship research, the term “cancer survivor” is broadly defined as any individual from the time of diagnosis through the remainder of life [
2]. In this study, breast cancer survivors were operationally defined as community-dwelling women who had completed primary treatment with curative intent and were undergoing routine surveillance and follow-up.
From January 3 to February 23, 2022, participants were recruited by convenience sampling from community-dwelling breast cancer survivors receiving care at the breast clinic of a university hospital in Daejeon, Korea. Eligibility criteria were as follows: (1) female sex, (2) age ≥19 years, (3) histologically confirmed breast cancer diagnosis, (4) completion of primary treatment with curative intent (surgery with or without adjuvant chemotherapy and/or radiotherapy), (5) current follow-up/surveillance status, (6) absence of secondary malignancies, (7) residence in the community (not hospitalized) with family members at the time of enrollment, and (8) sufficient Korean-language proficiency to understand and complete the self-report measures. Long-term adjuvant hormonal therapy, when applicable, was permitted because it is commonly administered during extended survivorship care. Conversely, individuals receiving active primary treatment (e.g., ongoing cytotoxic chemotherapy or radiotherapy for the initial diagnosis) were excluded to ensure a homogeneous post-treatment survivorship sample aligned with the study purpose.
The sample size was calculated using G*Power ver. 3.1.9.4. Assuming a significance level (α) of .05, statistical power (1–β) of .90, and a medium effect size (f²=.15) identified in a previous study of breast cancer survivors [
19], the minimum required sample size was 190, based on a conservative multiple regression model with up to 15 predictors, including the primary study variables and candidate sociodemographic and health-related covariates, and allowing for a 10% dropout rate. A total of 196 participants met the inclusion criteria and completed the survey. After exclusion of four incomplete responses, data from 192 participants were included in the final analysis.
1) Family functioning
Family functioning, defined as the participant’s perceived interactions with family members, was measured using the Family Adaptation, Partnership, Growth, Affection, and Resolve scale [
20]. The instrument consists of five items assessing adaptation, partnership, growth, affection, and resolve. Each item is rated on a 3-point Likert scale (0=hardly ever, 1=some of the time, 2=almost always), with total scores ranging from 0 to 10; higher scores indicate better family functioning. Internal consistency was Cronbach’s α=.80 in the original study [
20] and Cronbach’s α=.90 in the present study.
2) Motivation
Motivation for self-management was assessed using the Treatment Self-Regulation Questionnaire (TSRQ) [
21], which is grounded in SDT and designed to capture autonomous and controlled motivation. The TSRQ items were framed around engagement in daily self-management behaviors, including diet and exercise, and respondents were asked to indicate the extent to which each reason reflected why they engaged in these behaviors. The instrument comprised 19 items, including 8 assessing autonomous motivation (e.g., personal endorsement and intrinsic value) and 11 assessing controlled motivation (e.g., external pressure or obligation). Each item was rated on a 7-point Likert scale (1=not at all true to 7=very true). Mean scores were calculated for the two subscales. In the original validation study, the TSRQ subscales demonstrated acceptable internal consistency (Cronbach’s α), ranging from .85 to .93 for autonomous motivation, .74 to .86 for introjected regulation, and .73 to .91 for external regulation [
21]. In the present study, Cronbach’s α was .91 for autonomous motivation and .76 for controlled motivation (composite of introjected and external regulation).
3) Healthy behaviors
Healthy behaviors were measured using the Health-Promoting Lifestyle Profile II (HPLP-II) [
22]. The instrument comprises 52 items across six subdomains: health responsibility, physical activity, nutrition, spiritual growth, interpersonal relations, and stress management. Items are rated on a 4-point Likert scale (1=not at all to 4=always), and mean scores are calculated, with higher scores indicating greater engagement in healthy behaviors. The original HPLP-II demonstrated good internal consistency (Cronbach’s α=.94) [
22], and internal consistency in the present study was Cronbach’s α=.95.
4) Environmental mastery
Environmental mastery was measured using the Environmental Mastery subscale of the Psychological Well-Being Scale [
3,
23]. This scale assesses the subjective sense of control and efficacy in managing one’s life conditions and surrounding contexts, encompassing the various demands, resources, and circumstances encountered in daily life. It consists of eight items rated on a 6-point Likert scale (1=not at all true to 6=very true). Higher scores indicate a greater ability to manage and control one’s environment effectively. Internal consistency was Cronbach’s α=.82 in the original study [
3] and Cronbach’s α=.71 in the present study.
5) Sociodemographic and health-related characteristics
Sociodemographic characteristics included age, presence of a spouse (yes/no), educational level (high school or below vs. college or beyond), current employment status (yes/no), and monthly household income (measured in units of 10,000 Korean won [KRW]). Health-related characteristics included comorbidity, cancer treatment history, and subjective health status. Comorbidity was defined as the presence of at least one physician-diagnosed chronic condition (e.g., hypertension, diabetes, dyslipidemia, arthritis, or other chronic illnesses) and was coded dichotomously (yes/no). Cancer treatment history was assessed as a multiple-response item (mastectomy, chemotherapy, radiotherapy, hormonal therapy, targeted therapy, or other treatments). Subjective health status was assessed using a 5-point Likert scale (1=very poor to 5=very good).
4. Procedure
A research investigator stationed in the outpatient department approached potential participants and confirmed their willingness to participate. A breast cancer coordinator nurse then screened individuals who expressed interest to verify the absence of cancer recurrence or metastasis, after which they were enrolled in the study.
5. Ethical Considerations
This study was approved by the Institutional Review Board of Chungnam National University (No. 202101-SB-009-01). Participants were informed about the study purpose and procedures, the voluntary nature of participation, the assurance of anonymity, and the exclusive use of collected information for research purposes. They were also informed that they could discontinue participation at any time and withdraw from the study after completion without disadvantage. Data were collected after written informed consent was obtained, and participants completed the structured self-administered questionnaire in a quiet, private space within the center to ensure independent responses. Upon completion of the survey, participants received a KRW 5,000 gift voucher as a token of appreciation.
6. Statistical Analysis
Data were analyzed using IBM SPSS ver. 29.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize participants’ general characteristics, and the reliability of each measurement instrument was evaluated using Cronbach’s alpha coefficients. Pearson correlation analysis was conducted to examine the relationships among the main variables, including family functioning, motivation (autonomous and controlled), healthy behaviors, and environmental mastery.
Before the mediation analyses, key regression assumptions were evaluated. Multicollinearity among the independent variable (family functioning), mediators (autonomous or controlled motivation and healthy behaviors), and covariates (e.g., age, subjective health status, and cancer treatment history) was assessed using tolerance and variance inflation factor (VIF) statistics, with tolerance >.10 and VIF <10 as diagnostic thresholds [
24]. Independence of residuals was examined using the Durbin–Watson statistic, with values close to 2 indicating no first-order autocorrelation [
24]. Homoscedasticity was evaluated by examining residual plots for systematic patterns. All assumptions were adequately met, supporting the validity of the subsequent inferential analyses.
The serial mediation effects of motivation (autonomous and controlled) and healthy behaviors on the relationship between family functioning and environmental mastery were tested using Hayes’ PROCESS macro Model 6 for SPSS. PROCESS Model 6 provides estimates of the specific indirect effect for each mediating pathway as well as the total indirect effect, defined as the sum of all specific indirect effects. Accordingly, indirect effects by pathway (specific indirect effects) and the total indirect effect were reported separately. Statistical significance was evaluated using 5,000 bootstrap samples, and mediation effects were considered significant when the 95% confidence interval (CI) did not include zero.
RESULTS
1. Sociodemographic and Health-Related Characteristics and Their Association with Environmental Mastery
The mean age of the participants was 51.60 years (standard deviation [SD], 7.95 years), with a range of 32 to 69 years. Most participants had a spouse. Regarding educational attainment, 49.5% had a college degree or higher, whereas 50.5% had completed high school or less. Approximately 45.8% were currently employed, and 47.4% reported a monthly household income exceeding 4 million KRW.
Regarding health-related characteristics, 28.6% of participants reported having chronic diseases, and the mean subjective health status score was 3.06 (SD, 0.85; range, 1–5). For breast cancer treatment history, mastectomy was the most common treatment (86.5%), followed by hormonal therapy (36.5%), chemotherapy (4.7%), radiotherapy (2.6%), and targeted or other therapies (3.1%).
Environmental mastery differed significantly according to age (r=.25,
p=.001), subjective health status (r=.38,
p<.001), and history of chemotherapy (t=2.23,
p=.027) (
Table 1).
Pearson correlation analyses revealed significant associations among the key study variables (
Table 2). Family functioning was significantly correlated with autonomous motivation (r=.20,
p=.005), healthy behaviors (r=.44,
p<.001), and environmental mastery (r=.47,
p<.001). Healthy behaviors were significantly positively correlated with both autonomous motivation (r=.56,
p<.001) and controlled motivation (r=.17,
p=.020), as well as with environmental mastery (r=.56,
p<.001). Autonomous motivation was significantly correlated with environmental mastery (r=.32,
p<.001), and autonomous and controlled motivation were significantly correlated with each other (r=.39,
p<.001).
Multicollinearity diagnostics were acceptable, with tolerance values ranging from .55 to .99 and VIF values ranging from 1.02 to 1.83 [
24]. The Durbin–Watson statistic was 1.90, which is close to 2.0 and indicates negligible autocorrelation [
24]. Residual plots confirmed homoscedasticity. All regression assumptions were adequately met.
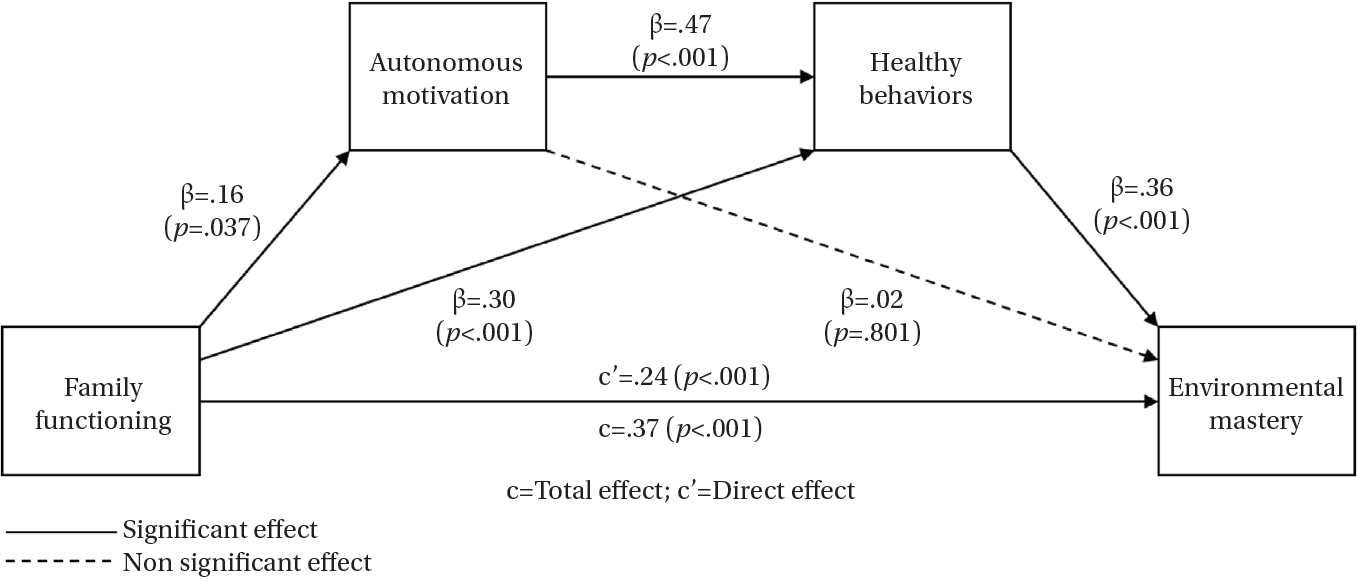
Table 3 presents the indirect and serial indirect effects of family functioning on environmental mastery through autonomous motivation and subsequent healthy behaviors. The sequential indirect effect through autonomous motivation and healthy behaviors was significant (standardized indirect effect, 0.03; 95% bootstrapped CI [BootCI], 0.00–0.06), indicating a serial mediation pathway. In addition, the indirect effect of family functioning on environmental mastery through autonomous motivation alone was not significant (standardized indirect effect, 0.00; 95% BootCI, −0.02 to 0.03), whereas the indirect effect through healthy behaviors was significant (standardized indirect effect, 0.11; 95% BootCI, 0.05–0.17).
Figure 1 illustrates the direct effect of family functioning on environmental mastery and the serial indirect effects through autonomous motivation and healthy behaviors. After adjustment for covariates (age, subjective health status, mastectomy, and chemotherapy), family functioning significantly predicted autonomous motivation (β=.16,
p=.037), healthy behaviors (β=.30,
p<.001), and environmental mastery (β=.24,
p<.001). Autonomous motivation significantly predicted healthy behaviors (β=.47,
p<.001) but not environmental mastery (β=.02,
p=.801), whereas healthy behaviors significantly predicted environmental mastery (β=.36,
p<.001).
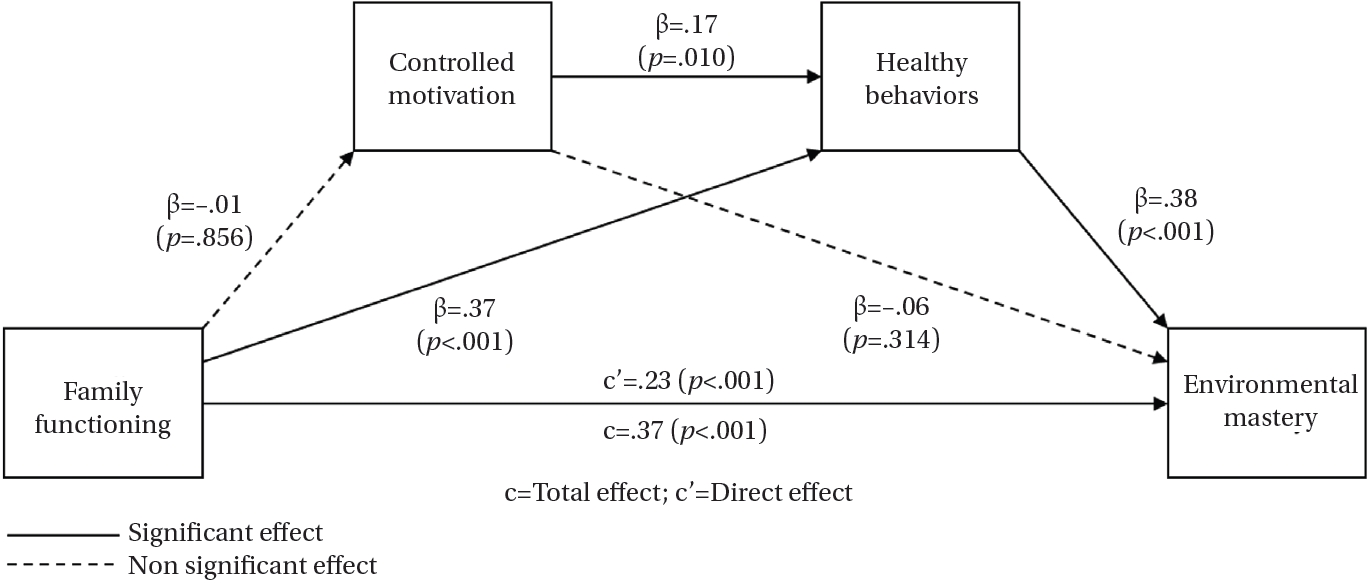
4. Serial Mediation Effects of Controlled Motivation and Healthy Behaviors in the Relationship between Family Functioning and Environmental Mastery
Figure 2 presents the direct and indirect effects of family functioning on environmental mastery through controlled motivation and healthy behaviors. After adjustment for covariates, family functioning did not significantly predict controlled motivation (β=−.01,
p=.856) but did significantly predict healthy behaviors (β=.37,
p<.001) and environmental mastery (β=.23,
p<.001). Controlled motivation significantly predicted healthy behaviors (β=.17,
p=.010) but not environmental mastery. This indicates that controlled motivation did not function as a mediator, whereas healthy behaviors remained a significant pathway linking family functioning to environmental mastery (
Table 3).
DISCUSSION
Understanding how breast cancer survivors actively manage their living environments and sustain environmental mastery throughout survivorship is essential for clarifying psychological well-being. Grounded in SDT, this study examined how family functioning was associated with environmental mastery through the serial mediating effects of autonomous and controlled motivation and healthy behaviors among breast cancer survivors.
A key finding was that family functioning was indirectly associated with environmental mastery through a sequential pathway involving autonomous motivation and healthy behaviors. This pattern is consistent with SDT’s proposition that supportive interpersonal contexts facilitate autonomous motivation, which in turn promotes engagement in healthy behaviors [
12,
16]. This finding is also consistent with evidence that adaptive family functioning is associated with greater autonomous motivation, healthier behaviors, and better psychological well-being [
8,
25]. Extending this literature, the present findings suggest a serial pathway linking family functioning to environmental mastery through autonomous motivation and healthy behaviors, thereby highlighting their relevance to survivors’ perceived capacity to manage and organize life circumstances.
Healthy behaviors emerged as a central mediator in the serial pathway. Family functioning showed a direct association with healthy behaviors beyond the motivational pathways, suggesting that families may facilitate healthy behaviors through additional mechanisms, such as practical assistance, encouragement, and behavioral modeling [
17,
18]. This interpretation is supported by evidence that family participation in decision-making and communication supports sustained engagement in healthy behaviors [
7,
9,
15]. Taken together, these findings suggest that supportive family environments may provide both emotional affirmation and concrete resources that help survivors establish healthy behaviors, thereby strengthening environmental mastery.
Consistent with SDT propositions and empirical evidence regarding the influence of motivation on behavioral engagement [
11,
12,
16], both autonomous and controlled motivation were associated with healthy behaviors. However, contrary to the initial expectation, neither autonomous nor controlled motivation independently mediated the association between family functioning and environmental mastery. Autonomous motivation contributed only as part of the serial pathway through healthy behaviors, indicating that self-endorsed motives may be necessary but not sufficient in the absence of behavioral enactment. This interpretation supports prior work showing that behavioral engagement is a key pathway linking motivational quality to psychological well-being [
13,
16]. In the present study, motivation was associated with environmental mastery primarily through engagement in healthy behaviors, underscoring the importance of behavioral implementation in survivors’ perceived environmental mastery. Notably, this finding differs from some previous studies in which motivational regulation showed more direct associations with well-being outcomes such as depression and anxiety [
13,
16,
26]. This difference may reflect the nature of the outcome examined. Environmental mastery, which encompasses the ability to manage and organize one’s living environment, may depend more on behavioral enactment than on motivational state alone.
In contrast, pathways involving controlled motivation were more limited than expected. Controlled motivation showed only a small association with healthy behaviors and was neither directly nor indirectly associated with environmental mastery. These findings are consistent with previous evidence indicating that controlled motivation (e.g., fear of recurrence, external pressure, perceived expectations) may support compliance-focused engagement in healthy behaviors but may be less likely to translate into sustained gains in psychological well-being or positive adaptation [
11,
13,
16,
26]. This pattern suggests that externally driven motivation may promote temporary compliance but has limited value for long-term adaptive outcomes related to environmental mastery. Taken together, these findings suggest that supportive family functioning may be most beneficial when it fosters autonomous motivation and enables sustained engagement in healthy behaviors.
Several limitations should be noted. First, the cross-sectional design precludes causal inference, and although healthy behaviors were modeled as antecedents of environmental mastery, reverse or reciprocal relationships are plausible. Longitudinal studies are needed to clarify temporal ordering. Second, the self-reported measures may be subject to recall and social desirability bias, and healthy behaviors were assessed as perceived engagement rather than with objective measures. Third, family functioning was assessed only from the survivors’ perspective, which limits insight into dyadic or systemic patterns. Previous research suggests that family members may hold divergent perceptions of family functioning [
9,
27] and that typological patterns, including supportive, conflictual, and intermediate traits [
9,
10,
14], may differentially predict outcomes. Future research should adopt longitudinal, multi-informant designs and incorporate objective measures of healthy behaviors and family functioning to clarify temporal and reciprocal relationships among the study variables. It would also be valuable to examine whether different family functioning profiles show distinct motivational and behavioral pathways to environmental mastery.
This study contributes to the literature by focusing on environmental mastery, a key dimension of long-term adaptation in cancer survivorship, and by delineating how family functioning, motivation, and healthy behaviors operate together in relation to this outcome. Autonomous motivation was associated with environmental mastery primarily through healthy behaviors, whereas controlled motivation showed limited influence on environmental mastery. These findings highlight the value of interventions that strengthen family functioning, foster autonomous motivation, and support sustained engagement in healthy behaviors as strategies to enhance environmental mastery among breast cancer survivors.
CONCLUSION
This study investigated the pathways linking family functioning with environmental mastery through autonomous and controlled motivation and healthy behaviors among breast cancer survivors. The main finding was that family functioning was indirectly associated with environmental mastery through a sequential pathway involving autonomous motivation and healthy behaviors, with healthy behaviors emerging as the primary mediator in this association. In contrast, controlled motivation contributed modestly to healthy behaviors but showed no association with environmental mastery, indicating that motivational quality, rather than its mere presence, may be central to positive psychological well-being in this population.
These findings suggest that enhancing environmental mastery among breast cancer survivors may require an integrated approach that strengthens family functioning, fosters autonomous motivation, and facilitates sustained engagement in healthy behaviors. Nursing practice should incorporate multicomponent interventions that engage families, support survivors’ autonomy, and promote adherence to healthy behaviors to enhance environmental mastery and long-term psychological well-being in breast cancer survivorship. Future research should evaluate family- and motivation-focused interventions and clarify how changes in family functioning, motivation, and healthy behaviors relate to changes in environmental mastery over time.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and design acquisition - HEY, SS, and HL; methodology - HEY and SS; investigation - SS and HL; formal analysis - HEY and SS; validation - HEY and SS; supervision - HEY; project administration - HEY; funding acquisition - HEY; drafting and critical revision of the manuscript - HEY, SS, and HL.
-
FUNDING
This study was supported by Chungnam National University Research Funds.
-
ACKNOWLEDGEMENT
None.
-
DATA AVAILABILITY STATEMENT
Participants did not provide consent for public open sharing of their individual-level data. Consequently, the datasets are not publicly available. De-identified data may be obtained from the corresponding author upon reasonable request, subject to institutional review and a data use agreement.
Figure 1.Serial mediation model of the association between family functioning and environmental mastery through autonomous motivation and healthy behaviors. Standardized regression coefficients are presented. Autonomous motivation (M1) and healthy behaviors (M2) were specified as serial mediators of the effect of family functioning on environmental mastery. Age, subjective health status, and cancer treatment history (mastectomy and chemotherapy) were included as covariates.
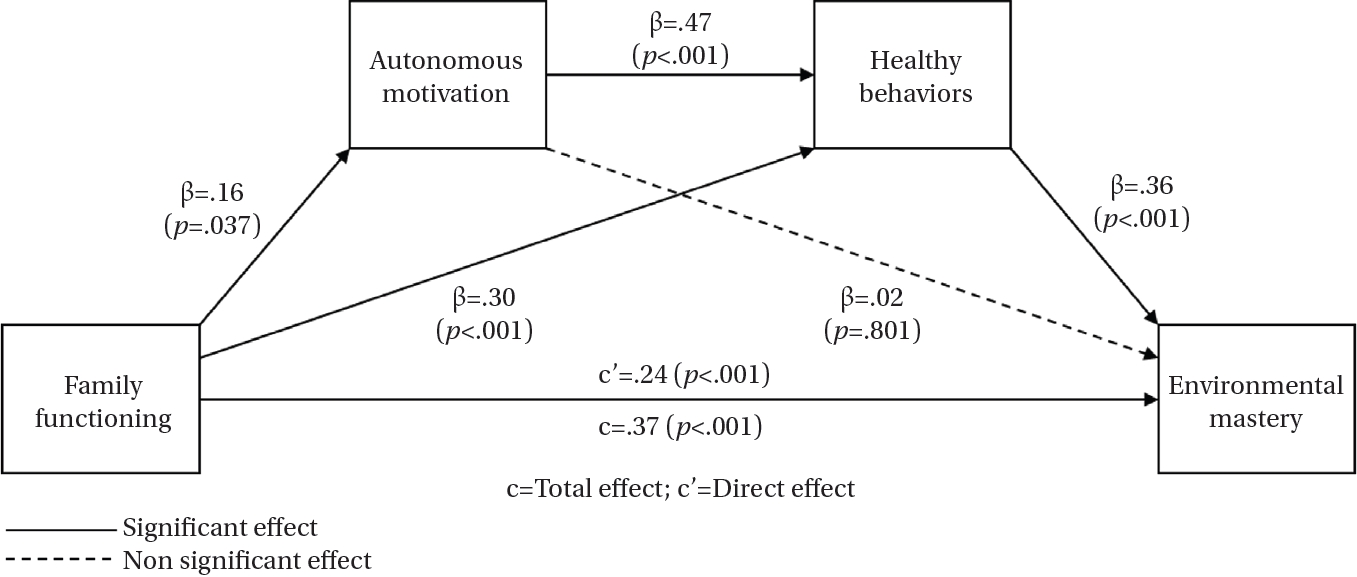
Figure 2.Serial mediation model of the association between family functioning and environmental mastery through controlled motivation and healthy behaviors. Standardized regression coefficients are presented. Controlled motivation (M1) and healthy behaviors (M2) were specified as serial mediators of the effect of family functioning on environmental mastery. Age, subjective health status, and cancer treatment history (mastectomy and chemotherapy) were included as covariates.
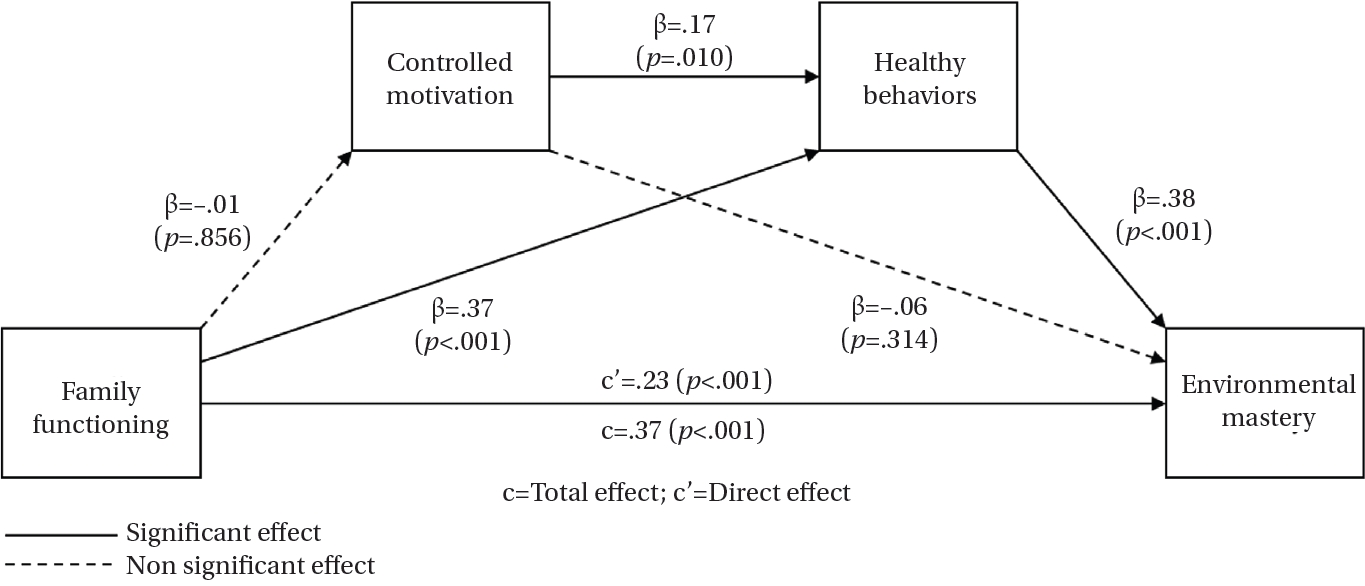
Table 1.Sociodemographic and Health-Related Characteristics of the Participants and Differences in Environmental Mastery (N=192)
|
Variables |
Categories |
M±SD or n (%) |
Environmental mastery |
|
t or r (p) |
|
Age (year) |
|
51.60±7.95 |
.25 (.001) |
|
Presence of a spouse |
Yes |
170 (88.5) |
–0.17 (.862) |
|
Educational level |
High school or below |
97 (50.5) |
0.40 (.693) |
|
College or beyond |
95 (49.5) |
|
|
Currently employed |
Yes |
88 (45.8) |
–1.16 (.249) |
|
Monthly household income (10,000 KRW) |
≤400 |
101 (52.6) |
–1.45 (.150) |
|
>400 |
91 (47.4) |
|
|
Subjective health status |
|
3.06±0.85 |
.38 (<.001) |
|
Comorbidity |
Yes |
55 (28.6) |
–0.32 (.752) |
|
Cancer treatment history |
Mastectomy |
166 (86.5) |
0.84 (.400) |
|
Hormonal therapy |
70 (36.5) |
–0.24 (.813) |
|
Chemotherapy |
9 (4.7) |
2.23 (.027) |
|
Radiotherapy |
5 (2.6) |
–0.48 (.635) |
|
Targeted or other therapies |
6 (3.1) |
–0.64 (.523) |
Table 2.Correlations among Main Study Variables (N=192)
|
Variables |
Mean ± SD |
1 |
2 |
3 |
4 |
|
r (p) |
|
1. Family functioning |
8.20 ± 2.39 |
- |
|
|
|
|
2. Autonomous motivation |
5.83 ± 1.17 |
.20 (.005) |
- |
|
|
|
3. Controlled motivation |
3.68 ± 1.34 |
-.00 (.988) |
.39 (<.001) |
- |
|
|
4. Healthy behaviors |
2.97 ± 0.48 |
.44 (<.001) |
.56 (<.001) |
.17 (.020) |
- |
|
5. Environmental mastery |
4.52 ± 0.71 |
.47 (<.001) |
.32 (<.001) |
-.00 (.962) |
.56 (<.001) |
Table 3.Specific and Total Indirect Effects of Family Functioning on Environmental Mastery through Motivation and Healthy Behaviors (N=192)
|
Indirect paths |
Standardized indirect effect |
BootSE |
95% BootCI |
|
Autonomous motivation |
|
|
|
|
Ind1: Family → Autonomous motivation → Environmental mastery |
0.00 |
0.01 |
–0.02 to 0.03 |
|
Ind2: Family → Healthy behaviors → Environmental mastery |
0.11 |
0.03 |
0.05 to 0.17 |
|
Ind3: Family → Autonomous motivation → Healthy behaviors → Environmental mastery |
0.03 |
0.02 |
0.00 to 0.06 |
|
Total indirect effect (sum of Ind1–Ind3) |
0.14 |
0.04 |
0.07 to 0.21 |
|
Controlled motivation |
|
|
|
|
Ind1: Family → Controlled motivation → Environmental mastery |
0.00 |
0.01 |
–0.01 to 0.02 |
|
Ind2: Family → Healthy behaviors → Environmental mastery |
0.14 |
0.04 |
0.08 to 0.22 |
|
Ind3: Family → Controlled motivation → Healthy behaviors → Environmental mastery |
0.00 |
0.00 |
–0.01 to 0.01 |
|
Total indirect effect (sum of Ind1–Ind3) |
0.14 |
0.04 |
0.08 to 0.22 |
REFERENCES
- 1. Brown J. Breast Cancer Research Foundation. Understanding breast cancer survival rates [Internet]. New York, NY: Breast Cancer Research Foundation; 2025 [cited 2025 December 18]. Available from: https://www.bcrf.org/about-breast-cancer/breast-cancer-survival-rates/
- 2. National Cancer Institute. Cancer stat facts: female breast cancer [Internet]. Bethesda, MD: National Cancer Institute; 2025 [cited 2025 December 18]. Available from: https://seer.cancer.gov/statfacts/html/breast.html
- 3. Ryff CD. Happiness is everything, or is it?: explorations on the meaning of psychological well-being. J Pers Soc Psychol. 1989;57(6):1069-81. https://doi.org/10.1037/0022-3514.57.6.1069
- 4. Gallagher MW, Long LJ, Richardson A, D'Souza JM. Resilience and coping in cancer survivors: the unique effects of optimism and mastery. Cognit Ther Res. 2019;43(1):32-44. https://doi.org/10.1007/s10608-018-9975-9
- 5. Sargent-Cox KA, Butterworth P, Anstey KJ. Role of physical activity in the relationship between mastery and functional health. Gerontologist. 2015;55(1):120-31. https://doi.org/10.1093/geront/gnu042
- 6. Lirola MJ, Hernandez-Rodriguez AI, Cuenca-Piqueras C, Prados-Megias ME. Resilience and renewal: the personal impact of physical activity in breast cancer survivors. BMC Womens Health. 2025;25(1):257. https://doi.org/10.1186/s12905-025-03791-3
- 7. Zhou T, Xiong W, Meng Z, Yu NX, Zhang J, Luo Y. Family resources and parental problem-solving skills mediate family functioning and family adaptation in families of children with cancer. J Clin Nurs. 2025;34(9):3704-19. https://doi.org/10.1111/jocn.17528
- 8. Tao L, Hu X, Fu L, Zhang X, Chen H. Effects of family beliefs and family strength on individual resilience and quality of life among young breast cancer survivors: a cross-sectional study. J Clin Nurs. 2023;32(11-12):2616-26. https://doi.org/10.1111/jocn.16321
- 9. Wang H, Yue H, Ren M, Feng D. Dyadic effects of family-functioning and resilience on quality of life in advanced lung cancer patients and caregivers: an actor-partner interdependence mediation model. Eur J Oncol Nurs. 2021;52:101963. https://doi.org/10.1016/j.ejon.2021.101963
- 10. Leow K, Lynch MF, Lee J. Social support, basic psychological needs, and social well-being among older cancer survivors. Int J Aging Hum Dev. 2021;92(1):100-114. https://doi.org/10.1177/0091415019887688
- 11. Patrick H, Williams GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. 2012;9:18. https://doi.org/10.1186/1479-5868-9-18
- 12. Deci EL, Ryan RM. The "What" and "Why" of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227-68. https://doi.org/10.1207/s15327965pli1104_01
- 13. Deci EL, Ryan RM. Facilitating optimal motivation and psychological well-being across life's domains. Can Psychol. 2008;49(1):14-23. https://doi.org/10.1037/0708-5591.49.1.14
- 14. Schuler TA, Zaider TI, Li Y, Hichenberg S, Masterson M, Kissane DW. Typology of perceived family functioning in an American sample of patients with advanced cancer. J Pain Symptom Manage. 2014;48(2):281-8. https://doi.org/10.1016/j.jpainsymman.2013.09.013
- 15. Lee JH, Kim HY. Symptom distress and coping in young Korean breast cancer survivors: the mediating effects of social support and resilience. J Korean Acad Nurs. 2018;48(2):241-53. https://doi.org/10.4040/jkan.2018.48.2.241
- 16. Ng JY, Ntoumanis N, Thogersen-Ntoumani C, Deci EL, Ryan RM, Duda JL, et al. Self-determination theory applied to health contexts: a meta-analysis. Perspect Psychol Sci. 2012;7(4):325-40. https://doi.org/10.1177/1745691612447309
- 17. Chang L, Zhang S, Yan Z, Li C, Zhang Q, Li Y. Symptom burden, family resilience, and functional exercise adherence among postoperative breast cancer patients. Asia Pac J Oncol Nurs. 2022;9(11):100129. https://doi.org/10.1016/j.apjon.2022.100129
- 18. Elshahat S, Treanor C, Donnelly M. Factors influencing physical activity participation among people living with or beyond cancer: a systematic scoping review. Int J Behav Nutr Phys Act. 2021;18(1):50. https://doi.org/10.1186/s12966-021-01116-9
- 19. Bae EJ, Kim YH. Mediation effects of basic psychological needs between autonomy support from healthcare providers and self-management among cancer survivors. Osong Public Health Res Perspect. 2019;10(6):385-93. https://doi.org/10.24171/j.phrp.2019.10.6.09
- 20. Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. 1982;15(2):303-11.
- 21. Levesque CS, Williams GC, Elliot D, Pickering MA, Bodenhamer B, Finley PJ. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ Res. 2007;22(5):691-702. https://doi.org/10.1093/her/cyl148
- 22. Walker SN, Sechrist KR, Pender NJ. The Health-Promoting Lifestyle Profile: development and psychometric characteristics. Nurs Res. 1987;36(2):76-81.
- 23. Kim M, Kim H, Cha K. Analyses on the construct of psychological well-being (PWB) of Korean male and female adults. Korean J Soc Pers Psychol. 2001;15(2):19-39.
- 24. Tabachnick BG, Fidell LS. Using multivariate statistics. 7th ed. Boston, MA: Pearson Education; 2019.
- 25. Zhong H, Li F, Xiao T, Liu C, Li Q, Li L, et al. How does family function affect the activation of patients with cancer anorexia undergoing chemotherapy?: a mixed methods study. Semin Oncol Nurs. 2025;41(3):151904. https://doi.org/10.1016/j.soncn.2025.151904
- 26. Ntoumanis N, Ng JY, Prestwich A, Quested E, Hancox JE, Thogersen-Ntoumani C, et al. A meta-analysis of self-determination theory-informed intervention studies in the health domain: effects on motivation, health behavior, physical, and psychological health. Health Psychol Rev. 2021;15(2):214-44. https://doi.org/10.1080/17437199.2020.1718529
- 27. Ochoa CY, Cho J, Miller KA, Baezconde-Garbanati L, Chan RY, Farias AJ, et al. Hispanic/Latinos and non-Hispanic whites' childhood cancer survivors and parents: a dyadic analysis of coping resources and mental health. J Cancer Surviv. 2024;18(3):996-1005. https://doi.org/10.1007/s11764-023-01339-8


 E-SUBMISSION
E-SUBMISSION
